Hansol Chang: Department of Emergency Medicine, Sungkyunkwan University School of Medicine, Seoul, Republic of Korea; Department of Digital Health, Samsung Advanced Institute for Health Science & Technology (SAIHST), Seoul, Republic of Korea.
Seok Goo Kim: Department of Emergency medicine, Dongsuwon General Hospital, Gyeonggi-do, Repubulic of Korea.
IkJoon Jo: Department of Emergency Medicine, Sungkyunkwan University School of Medicine, Seoul, Republic of Korea.
* Hee Yoon: Department of Emergency Medicine, Sungkyunkwan University School of Medicine, Seoul, Republic of Korea.
Background: The current Cardiopulmonary Resuscitation (CPR) guidelines recommend a cardiac rhythm check every 2 min to evaluate the Return of Spontaneous Circulation (ROSC). Central artery pulse checks are generally performed manually when an organizing rhythm is recognized on the monitor, but several studies have shown that this method is not reliable. Recently, a case series of a novel approach can be used to determine the presence or absence of pulses using direct Point-of-Care Ultrasound (POCUS) compression of the central arteries.
Case Presentation: An 87-year-old female patient was transported to the emergency department in a cardiac arrest state. While performing CPR according to the Advanced Cardiovascular Life Support guidelines, we assessed the pulse by direct POCUS compression of the carotid artery using an ultrasound probe. During the third cycle of chest compression, the carotid artery’s collapse caused by probe compression was no longer observed while the vein still collapsed. Then, at the 6 min rhythm check, the carotid artery pulse was palpable manually, and ROSC was confirmed.
Conclusion: Thus, we assessed the efficacy of bedside POCUS in a case to evaluate carotid artery compressibility during chest compression to rapidly assess the ROSC.
Introduction
Point-of-Care Ultrasound (POCUS) is a core application of emergency medicine and is frequently used to guide resuscitation [1,2]. POCUS is used to improve the quality of chest compressions, identify the reversible causes of cardiac arrest, and predict short-term survival based on visible cardiac activity [3–5]. Recent studies have aimed to determine the Return of Spontaneous Circulation (ROSC) by detecting blood flow using carotid artery ultrasonography. Moreover, Simard et al. presented a case series indicating a new method for assessing the carotid artery’s compressibility during rhythm check assessment in the same way as verifying deep vein thrombosis with ultrasonography [6]. Thus, this study aimed to demonstrate the efficacy of bedside POCUS in a case for the evaluation of carotid artery compressibility during chest compressions to rapidly assess ROSC.
Case Presentation
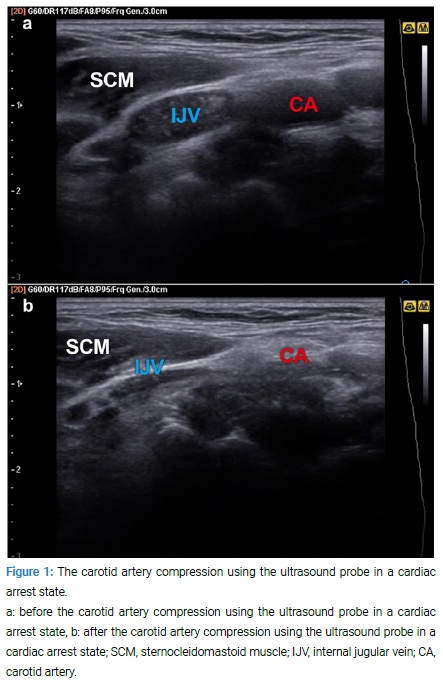
An 87-year-old woman in a cardiac arrest state was transported to our emergency department in an ambulance. Cardiopulmonary Resuscitation (CPR) was performed according to the Advanced Cardiovascular Life Support guidelines of the American Heart Association (AHA), and ROSC was evaluated by first assessing carotid artery manual pulsation [7]. One of the physicians attempted to evaluate ROSC by performing carotid artery ultrasonography. During CPR, he began the assessment by directly compressing the carotid artery using an ultrasound probe; then, compressibility was evaluated in real-time. In the beginning, the physician completely compressed the carotid artery using the probe during chest compression (Video 1*, Figure 1).
Video 1:The carotid artery compression using the ultrasound probe during chest compression in a cardiac arrest state.
After 2 min, the carotid artery clearly collapsed during a pulse check assessment (Video 2*).
Video 2: The carotid artery compression using the ultrasound probe at the pulse check time in a cardiac arrest state.
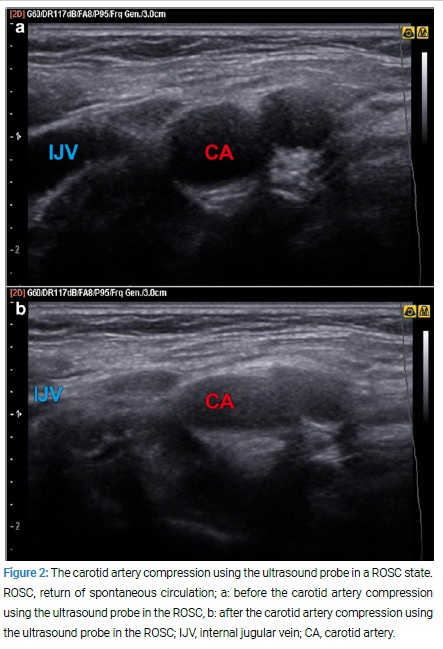
However, during the third cycle of chest compression, the carotid artery’s collapse caused by probe compression was no longer observed while the vein still collapsed (Video 3*, Figure 2).
Video 3: The carotid artery compression using the ultrasound probe during chest compression in the ROSC.
Therefore, the physician believed that ROSC was achieved and began to prepare for post-resuscitation care in the next cycle. During the 6-min rhythm check, the carotid artery did not collapse. However, the vein still collapsed due to probe compression (Video 4*). An organized rhythm was also seen on the electrocardiogram monitor, and the carotid artery pulse was palpable manually. Finally, ROSC was confirmed.
Video 4: The carotid artery compression using the ultrasound probe at the pulse check time in the ROSC.
Discussion
During CPR, an accurate rhythm check is important in managing a cardiac arrest patient because arrest algorithms rely on the cardiac rhythm when determining the appropriate treatment pathway. The AHA guidelines recommend a cardiac rhythm check every 2 min to evaluate the ROSC, and central arterial pulse checks are usually performed manually when an organized rhythm is displayed on the monitor [7]. Different studies have shown that manual detection of a pulse is not reliable within the last three decades, with a significant rate of prolonged pulse checks extending beyond the recommended time of 10 sec [8–11]. Therefore, the AHA removed pulse checks from lay rescuer training guidelines in 2015 [12]. We applied bedside POCUS compression of the carotid artery during CPR in a cardiac arrest patient in the current case. Thus, ROSC can be rapidly assessed before the rhythm check assessment.
In addition to the manual pulse check during CPR, noninvasive methods, including end-tidal carbon dioxide (ETCO2) or arterial line (A-line) monitoring, can be used to check a pulse. Although A-line monitoring can provide useful information for detecting ROSC, achieving an A-line requires some time, particularly in cases of out-of-hospital cardiac arrest [13]. ETCO2 monitoring may be another option. However, the patient must be intubated, and specific monitoring equipment is required. Moreover, airway secretion may be affected, and there are no accurate standard values for ROSC [14,15].
To date, the application of POCUS in cardiac arrest has primarily focused on the presence of cardiac standstill and the diagnosis of the reversible causes of cardiac arrest. Some studies have recently assessed alternative methods for manual pulse check using ultrasonography [16,17]. Focused cardiac ultrasound during CPR can directly assess cardiac activity. However, it should be examined during the rhythm check assessment when chest compression is stopped. Therefore, the hands-off time may be delayed, and the physician may require more training to obtain an accurate view [4,18]. Some studies have used Doppler ultrasonography for pulse check or the measurement of central blood flow velocity [16,19]. However, the relative movement between the transducer and skin induced by chest compression causes challenges in maintaining blood flow measurements during resuscitation.
Simard et al. showed another pulse check method that can accurately identify cardiac arrest through POCUS compression of the central arteries in a case series [6]. Using this technique, they found that a POCUS pulse check can be consistently performed within <5 sec and that it can be clearly identified even when palpation yields indeterminate results. The evaluation of the carotid artery’s collapsibility is a noninvasive and rapid method used to determine the presence or absence of pulses. In addition, this method is extremely effective because it can be easily performed at the bedside without posture limitation during chest compression. In our case, ROSC could be recognized during chest compression before the rhythm check time. Even if chest compression is performed, the cardiac output is between 20% and 40% compared to that before the arrest state [20,21]. Therefore, we assumed that if there is no effective blood flow in the central artery during chest compression, then the artery would be completely compressed; otherwise, ROSC is achieved. This method was applied to cardiac arrest patients, and ROSC was rapidly observed during chest compression.
The presence or absence of a pulse is a critical factor when managing critically ill and unresponsive patients, and it is used to determine an appropriate resuscitation algorithm for cardiac arrest. In addition, if ROSC can be identified during chest compressions, then the next step of treatment can be determined more rapidly, and patients can be prepared for post-resuscitation care. However, only a few studies and case reports have used this method. Therefore, if there are a higher number of cases and clinical trials, the POCUS carotid pulse check can be used as an alternative to the manual pulse check. Thus, further clinical studies must be conducted to validate this finding.
Conclusion
In the current case, bedside POCUS was applied to a cardiac arrest patient, and ROSC was confirmed during chest compression through ultrasound compression of the carotid artery.
Declarations
Ethics Approval and Consent to Participate: The study was approved by the Institutional Review Board of Samsung Medical Center (IRB File Number: 2019-08-090). The need for informed consent was waived given the study’s observational and anonymous nature.
Consent for Publication: All authors agree with consent for publication.
Availability of data and Material: The datasets supporting the conclusions of this article are included within the article.
Competing Interests: The authors declare no conflict of interest.
Funding: This research received no external funding.
Author Contributions: Jo IJ: Conceptualization; Yoon H, Kim SG, Jo IJ: Methodology; Jo IJ: Data Curation; Chang H, Yoon H: Writing – Original Draft Preparation; Chang H, Kim SG, Yoon H, Jo IJ: Writing – Review and Editing; Jo IJ, Yoon H: Supervision.
References
Ultrasound Guidelines: Emergency, Point-of-Care and Clinical Ultrasound Guidelines in Medicine. Ann Emerg Med. 2017;69(5):E27–E54.
Long B, Alerhand S, Maliel K, Koyfman A. Echocardiography in cardiac arrest: An emergency medicine review. Am J Emerg Med. 2018;36(3):488–493.
Blanco P, Martinez Buendia C. Point-of-care ultrasound in cardiopulmonary resuscitation: a concise review. J Ultrasound. 2017;20(3):193–198.
Lalande E, Burwash-Brennan T, Burns K, Atkinson P, Lambert M, Jarman B, et al. Is point-of-care ultrasound a reliable predictor of outcome during atraumatic, non-shockable cardiac arrest? A systematic review and meta-analysis from the SHoC investigators. Resuscitation. 2019;139:159–166.
Blyth L, Atkinson P, Gadd K, Lang E. Bedside focused echocardiography as predictor of survival in cardiac arrest patients: a systematic review. Acad Emerg Med. 2012;19(10):1119–1126.
Simard RD, Unger AG, Betz M, Wu A, Chenkin J. The pocus pulse check: a case series on a novel method for determining the presence of a pulse using point-of-care ultrasound. J Emerg Med 2019;56(6):674–679.
Link MS, Berkow LC, Kudenchuk PJ, Halperin HR, Hess EP, Moitra VK, et al. Part 7: Adult Advanced cardiovascular life support: 2015 american heart association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2015;132(18 Suppl 2):S444–S464.
Eberle B, Dick WF, Schneider T, Wisser G, Doetsch S, Tzanova I. Checking the carotid pulse check: diagnostic accuracy of first responders in patients with and without a pulse. Resuscitation. 1996;33(2):107–116.
Ochoa FJ, Ramalle-Gomara E, Carpintero JM, Garcia A, Saralegui I. Competence of health professionals to check the carotid pulse. Resuscitation. 1998;37(3):173–175.
Lapostolle F, Le Toumelin P, Agostinucci JM, Catineau J, Adnet F. Basic cardiac life support providers checking the carotid pulse: performance, degree of conviction, and influencing factors. Acad Emerg Med. 2004;11(8):878–880.
Dick WF, Eberle B, Wisser G, Schneider T. The carotid pulse check revisited: what if there is no pulse? Crit Care Med. 2000;28(11 Suppl):N183–N185.
Kleinman ME, Brennan EE, Goldberger ZD, Swor RA, Terry M, Bobrow BJ, et al. Part 5: Adult basic life support and cardiopulmonary resuscitation quality: 2015 american heart association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2015;132(18 Suppl 2):S414–S435.
Lipps J, Goldberg A, DeMaria S, Khelemsky Y, Levine A, Yildiz V, et al. Presence of an arterial line improves response to simulated hypotension and pulseless electrical activity. J Clin Monit Comput. 2017;31(5):911–918.
Pantazopoulos C, Xanthos T, Pantazopoulos I, Papalois A, Kouskouni E, Iacovidou N. A review of carbon dioxide monitoring during adult cardiopulmonary resuscitation. Heart lung circ. 2015;24(11):1053–1061.
Turle S, Sherren PB, Nicholson S, Callaghan T, Shepherd SJ. Availability and use of capnography for in-hospital cardiac arrests in the United Kingdom. Resuscitation. 2015;94:80–84.
Zengin S, Gumusboga H, Sabak M, Eren SH, Altunbas G, Al B. Comparison of manual pulse palpation, cardiac ultrasonography and Doppler ultrasonography to check the pulse in cardiopulmonary arrest patients. Resuscitation. 2018;133:59–64.
Kucewicz JC, Salcido DD, Adedipe AA, Truong K, Nichol G, Mourad PD. Towards a non-invasive cardiac arrest monitor: An in vivo pilot study. Resuscitation. 2019;134:76–80.
Huis In ‘t Veld MA, Allison MG, Bostick DS, Fisher KR, Goloubeva OG, Witting MD, et al. Ultrasound use during cardiopulmonary resuscitation is associated with delays in chest compressions. Resuscitation. 2017;119:95–98.
Germanoska B, Coady M, Ng S, Fermanis G, Miller M. The reliability of carotid ultrasound in determining the return of pulsatile flow: A pilot study. Ultrasound. 2018;26(2):118–126.
Andreka P, Frenneaux MP. Haemodynamics of cardiac arrest and resuscitation. Curr Opin Crit Care. 2006;12(3):198–203.
Luce JM, Ross BK, O’Quin RJ, Culver BH, Sivarajan M, Amory DW, et al. Regional blood flow during cardiopulmonary resuscitation in dogs using simultaneous and nonsimultaneous compression and ventilation. Circulation. 1983;67(2):258–265.
Chang H, Kim SG, Jo I, Yoon H. Use of carotid artery compressibility detected on ultrasonography during chest compression to validate return of spontaneous circulation. Clin Case Rep J. 2020;1(7):1–4.
Clinical Case Reports Journal is the state-of-the-art platform to showcase medical journals across scientific community and a one-stop solution for publishing the manuscripts of varied medical specialities.
Main Links
Useful Links
Our Contacts
Clinical Case Reports Journal,
C/O Infact Publications LLC,
16192 Coastal Highway,
Lewes, Delaware 19958 USA