Abstract
Introduction: In Africa, hernia is a common disease, with the majority resulting from chronic increase in intra-abdominal pressure from laboring work. A few cases have been reported resulting from trauma.
Case Presentation: A 26-year-old male presented with a reducible left iliac fossa swelling following a road traffic accident. A diagnosis of traumatic abdominal wall hernia was made, and he had exploration and repair of the defect with mesh. Post-operative recovery was uneventful.
Conclusion: Trauma is a rare but known cause of abdominal wall hernia and requires a high index of suspicion for diagnosis.
Introduction
Abdominal wall hernia is one of the most prevalent surgical conditions in Africa [1–4]. It is commonly caused by repeated increases in intra-abdominal pressure due to chronic laboring jobs [5]. Road traffic accidents are common causes of injury worldwide, with the majority of injuries affecting the external limbs [6]. In rare instances, abdominal wall hernia may occur following abdominal wall trauma, disrupting the wall integrity. The lower abdominal wall is weaker and has natural orifices like the inguinal canal. Hence, traumatic abdominal wall hernia is common in this location [7]. We present a case of acute abdominal wall hernia due to a road traffic accident.
Case Presentation
A 26-year-old male, who was riding a motorbike, collided with a moving car at a low velocity. He fell off the motorbike, hitting his left lower abdomen on the ground, with no loss of consciousness but pain in the left lower quadrant of the abdominal wall.
Following the accident, he was brought to the hospital for assessment. Upon evaluation, it was noticed that he had a reducible swelling in the left lower quadrant of the abdominal wall, which was caused by a cough impulse. The skin was abrased overlying the swelling, with mild tenderness over the area but no signs of peritonitis. No other injuries were detected (Figure 1).

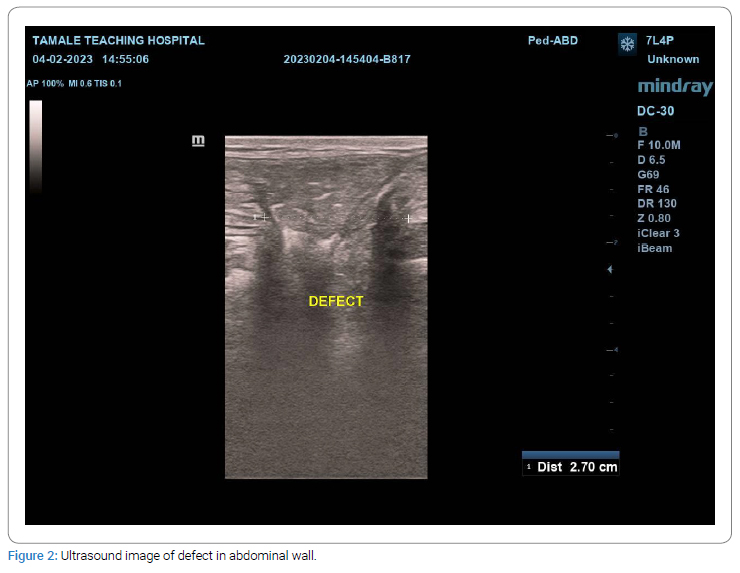
An ultrasound scan confirmed the presence of bowel loops in the subcutaneous space with an abdominal wall defect measuring 2.7 cm wide. There was no intra-abdominal collection seen. A diagnosis of traumatic abdominal wall hernia was made (Figure 2).
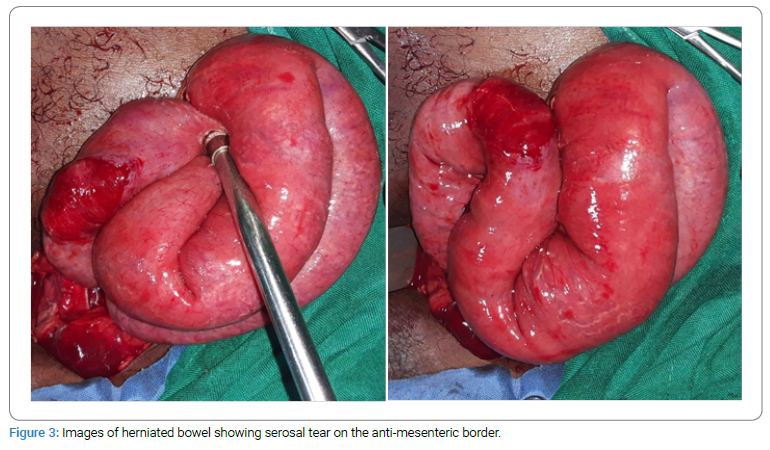
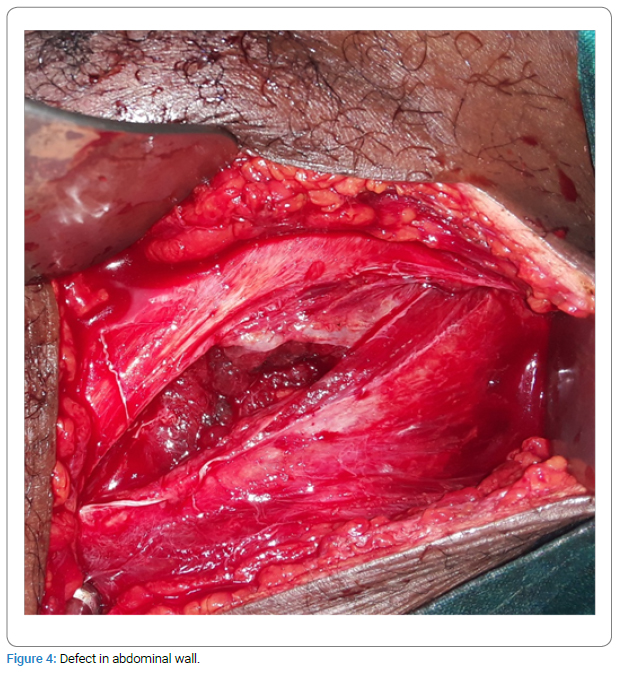
Intraoperative exploration of the left lower quadrant, where the swelling was located, revealed approximately 15 cm of ileum herniating through the abdomen wall (Figure 3), with a defect measuring 7 cm in length and 3 cm in width (Figure 4). There was a mild contusion of the mesentery of the herniated bowel with a 2 cm x 2 cm serosal tear on the anti-mesenteric border (Figure 3). The rest of the small bowel was inspected, and no other injuries were found. Only minimal subcutaneous tissue and muscle contusion were seen during the exploration.
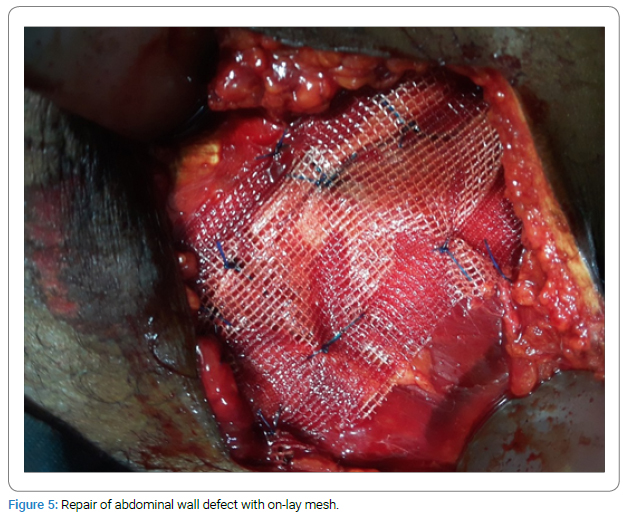
The serosal tear was repaired with Vicryl 3/0, and the bowel was reduced. Muscles at the defect site were closed with Vicryl 0, and the fascial defect was repaired with an onlay mesh (Figure 5). Skin closure was done with nylon 2/0.
The post-operative period was uneventful, and the surgical wound healed without complications (Figure 6).

Discussion
Trauma is a rare but known cause of abdominal wall hernia, with the earliest report dating back to 1906 [8]. The tangential force of the trauma easily produces shearing stresses to the underlying muscles, fascia, and peritoneum, while the skin is usually preserved as it is more elastic [9].
In some instances, associated hematoma may confound the diagnosis, and thus, a high index of suspicion is required to make the diagnosis [10]. In some reports, children are the usual culprits sustained by trauma due to bicycle-handle bars. This is thought to be due to the relatively weak fascia of children and their more elastic skin [11–13]. Our case was much older, and perhaps the impact of the fall was strong enough to disrupt the tissues of the abdominal wall.
Diagnosis of traumatic abdominal wall hernia is clinical; however, imaging helps to identify the size of the defect as well as associated visceral injuries. Computed Tomography (CT) scan is deemed the best imaging modality in the diagnosis of traumatic abdominal wall hernia and also associated injuries [10,14,15]. CT scan is a helpful tool to suggest bowel injury in blunt traumas since the presence of bowel-wall thickening, free fluid, mesenteric infiltration, or free air is alarming for bowel injury [16]. However, in a low-resource environment like ours, this is much more costly to carry out; thus, our choice of ultrasound scan was followed by an exploration of the defect site. Alternative to a CT scan, evaluating traumatic abdominal hernia in a stable patient in developing countries could be a small bowel follow-through with water-soluble contrast [7].
The modalities of treatment of traumatic abdominal wall hernia vary among authors with no consensus [11–13,17]. In a stable patient with no associated injuries, conservative treatment with the use of a cloth corset has been reported without the need for exploration [18]. Delayed repair can be done if a CT scan is available and confirms that there are no associated injuries or bowel strangulation.
Other authors have advocated for immediate exploration to avoid visceral incarceration, as well as in a stable patient [19]. Considering our setting where available theatre space and logistics are not always guaranteed, we found it necessary to do exploration and immediate repair in this case.
Both primary repair of the defect and the use of mesh have been described [11–13,17]. In a meta-analysis by Karhof et al., the number of hernia recurrences after primary repair was higher than that of those who had mesh repair, though this was not statistically significant. Considering that a majority of people in our environment engage in labor-intensive jobs, we deemed it necessary to do mesh repair to avert any recurrence.
Conclusion
Trauma is a rare but known cause of abdominal wall hernia. Thus, during our evaluation of a trauma patient, a high index of suspicion is required in order to diagnose this condition.
Conflict of Interest
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Informed consent was obtained for this publication.
Keywords
Acute abdominal wall hernia; Trauma; Accident
Cite this Article
Muntaka AJM, Bawa AA, Tabiri S, Baba AB. Acute abdominal wall hernia due to trauma: a case report in northern ghana. Clin Case Rep J. 2024;5(1):1–5.
Copyright
© 2024 Abdul-Jalilu Mohammed Muntaka. This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY-4.0).
