Abstract
Introduction: Contralateral obstruction from a giant megaureter is a rare cause of bilateral hydronephrosis. Most cases have been reported in children, with the oldest reported case being a 15-year-old.
Case presentation: A 23-year-old female para 1 presenting with right-sided pyoureteronephrosis due to a giant megaureter, causing left-sided hydronephrosis. We had a nephrostomy insertion followed by a right nephro-ureterectomy.
Introduction
Bilateral hydronephrosis usually results from obstruction of the lower urinary tract with back pressure affecting both kidneys. It may also be due to obstruction of both upper urinary tracts from causes such as ureteric calculi or bilateral pelvi-ureteric junction obstruction.
Rarely, contralateral obstruction from a megaureter may present with bilateral hydronephrosis. This is usually congenital and thus may be detected in utero or in childhood, when treatment may be given. In a low-resource area with relatively poor health service, these abnormalities are detected much later in life, often due to complications caused by the condition. We report a case of right-sided giant megaureter from distal ureteric stenosis presenting with pyonephrosis on the affected side and contralateral hydronephrosis due to compression on the contralateral ureter.
Case Presentation
The case is a 23-year-old female, Para 1, from a rural community in northern Ghana, who presented with a right flank mass, fever, and chills. She had been having recurrent right flank pain from childhood, for which she had been seeking herbal treatment. On examination, she was febrile with a temperature of 38.8 degrees Celsius, pulse rate of 92 bpm regular, Blood pressure of 100/60 mmg, and moderately pale. Abdominal examination revealed a tender mass in the right flank.
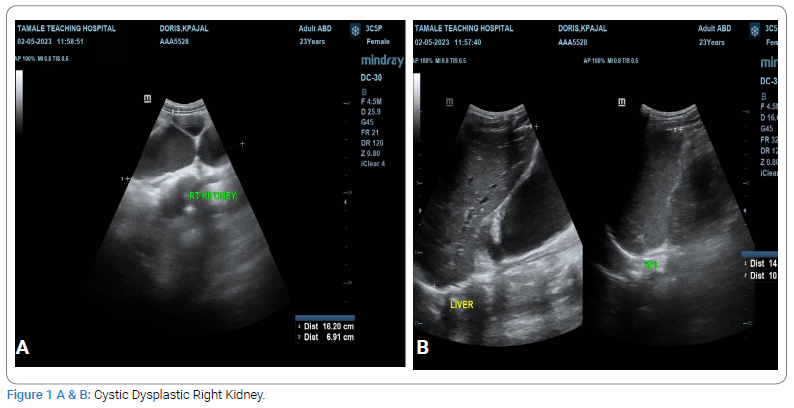
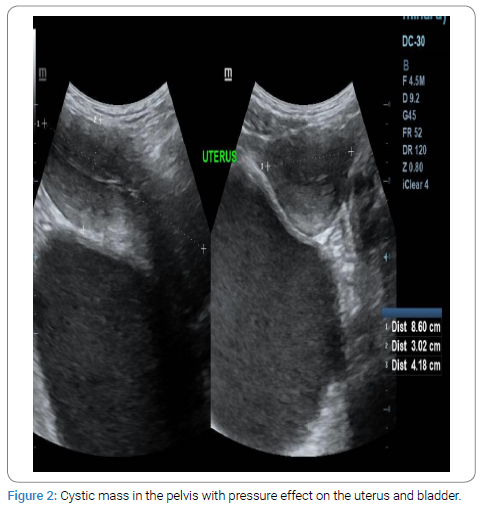
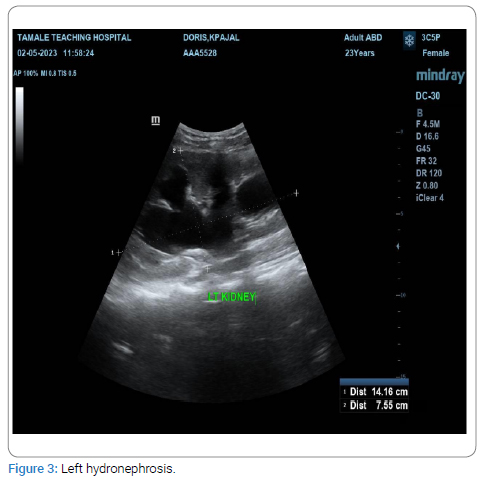
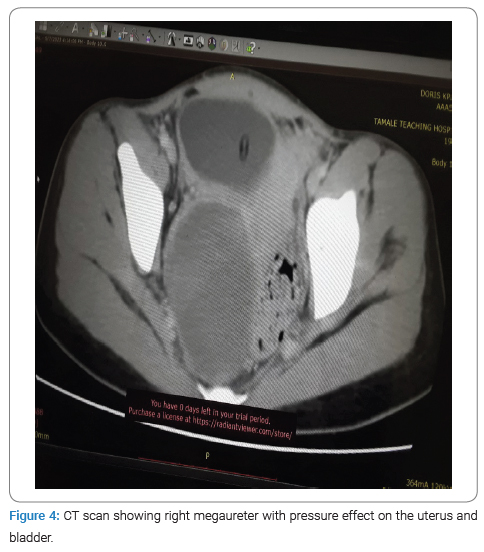
An ultrasound scan revealed severe right hydronephrosis with cortical thinning and a cystic mass in the right pelvis, displacing the uterus and bladder to the left (Figure 1,Figure 2). There was also moderate left hydronephrosis (Figure 3). A computerized Tomography scan revealed a right-sided megaureter with distal obstruction and severe right hydronephrosis in a nonfunctioning Kidney. There was also moderate left hydronephrosis due to contralateral obstruction from the right megaureter (Figure 4).
Bilateral nephrostomy tubes were placed with 1700 ml of purulent drainage on the right and 1100 ml of clear effluent on the left, over 24 hours. Intravenous antibiotics and analgesics were also given.
A week later, when the fever subsided, the patient underwent exploratory laparotomy. The findings included a dysplastic right kidney with right ureteral dilation massive at the distal part. There was a stricture close to the right uretero-vesical junction (Figure 5). A right nephro-ureterectomy was done. The left ureter was identified, and dye was instilled through the nephrostomy tube to assess for patency after the right nephro-ureterectomy. The dye was seen in the urethral catheter draining the bladder, indicating that the left ureter was patent. Post-operative ultrasound was performed seven days after surgery and showed resolution of the hydronephrosis on the left side (Figure 6).


Discussion
Giant megaureter is a rare congenital abnormality first reported in 1964 by Chatterjee [1]. The pathology is usually due to complete obstruction of the ureter in fetal life [2]. Like most other congenital anomalies, it is usually detected in utero or in early childhood. Thus, most cases have been reported among children, with the oldest published case report being of a 15-year-old teenager [3].
It is thought that muscular dysplasia at the distal ureter may account for this anomaly, though sometimes distal ureteral atresia may be the cause [4]. This results in stasis within the ureter and kidney.
Our case was a 21-year-old woman, far older than the usual age of detection and treatment. This could possibly be due to the low socioeconomic background and the poor health service in our environment. Another contributing factor is the patient’s prior childbirth, which could have caused acquired obstruction due to iatrogenic damage or an otherwise traumatic delivery. The physiology of pregnancy could also have exacerbated previously subclinical obstruction due to the increased glomerular filtration rate and fluid retention [5].
Most patients present with an abdominal mass; rarely, they may also present with contralateral ureteric obstruction [3], compression of the inferior vena cava [6], or even bowel obstruction [7]. Our patient presented with an abdominal mass and contralateral ureteric obstruction. Because of the long-standing nature of the hydronephrosis, there was a secondary infection presenting as pyonephrosis.
CT scan, when available, is the best modality in making the diagnosis of a patient presenting with an abdominal mass. Our patient had an ultrasound, which was suggestive, with a subsequent CT scan performed to confirm the diagnosis.
In a segmental giant megaureter with preserved renal function, excision of the dilated part followed by uretero-ureterostomy may be done [8]. However, nephro-ureterectomy is the treatment choice for a totally dilated ureter with a dysplastic non-functioning kidney. Our patient had a dysplastic, non-functioning left kidney with pyoureteronephrosis, and a nephro-ureterectomy was done.
The case illustrates some of the challenges that face rural and medically underserved communities globally, leading to atypical presentations that may prevent or delay diagnosis and treatment. Clinicians serving these populations must be prepared to broaden their differential diagnoses beyond classic teachings originating from urban academic practices.
Conflict of Interest
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Informed consent was obtained for this publication.
Keywords
Contralateral obstruction; Giant megaureter; Hydronephrosis
Cite this article
Muntaka AJM, Yenli EMT, Fuseini I, Awe BW, Barlow L. Right sided pyoureteronephrosis due to a giant megaureter causing left-sided hydronephrosis in a 23-year-old para 1: a case report. Clin Case Rep J. 2024;5(3):1–4.
Copyright
© 2024 Abdul-Jalilu Mohammed Muntaka. This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY-4.0).
