Empedobacter brevis Bacteremia: A Rare Case Report From India
* Sharma A;
Randhawa VS;
Shalu Gupta;
-
* Sharma A: Department of Microbiology, Lady Hardinge Medical College, New Delhi, India
-
Randhawa VS: Department of Microbiology, School of Medical Sciences and Research, Sharda University, Greater Noida 201310, Uttar Pradesh, India
-
Shalu Gupta: Neonatologist, Kalawati Saran Children’s Hospital, Lady Hardinge Medical College, New Delhi, India
Abstract
Empedobacter brevis, previously known as Flavobacterium brevis, is a Gram-negative, short, non-motile rod, which is widely distributed in the environment, both in soil and water. E. brevis has also been found in the hospital environment, leading to cases of nosocomial infections. E. brevis, though considered rarely pathogenic, is reported to cause cutaneous infections, meningitis, pneumonia, septicaemia, endophthalmitis, and ventricular-associated infections. We report here a case of a 2-year-old male child who presented in emergency with status epilepticus with a past history of Severe Acute Malnutrition (SAM) and gastroenteritis, and developing sepsis caused by Empedobacter brevis. Awareness regarding this uncommon pathogen is important to minimize morbidity and mortality.
Abbreviations
SAM: Severe Acute Malnutrition; PICU: Paediatric Intensive Care Unit; GCS: Glasgow Coma Scale; LFT: Liver Function Test; KFT: Kidney Function Test; CSF: Cerebrospinal Fluid; CECT: Contrast Enhanced Computed Tomography; TTG: Tissue Transglutaminase; HIV: Human Immunodeficiency Virus; BAL: Bronchoalveolar Lavage; LFA: Lateral Flow Assay; RT-PCR: Real Time-Polymerase Chain Reaction; ARDS: Acute Respiratory Distress Syndrome; DIC: Disseminated Intravascular Coagulation; AKI: Acute Kidney Injury; MODS: Multi Organ Dysfunction Syndrome
Introduction
Empedobacter brevis is a Gram-negative, non-motile bacillus, an obligate aerobe that rarely causes infection in humans [1]. The reservoir of these bacteria is in the environment, such as soil, plants, water, food, hospital water sources, including incubators, sinks, faucets, tap water, haemodialysis systems, saline solutions, and other pharmaceutical solutions [2]. We present here the first case report of sepsis caused by Empedobacter brevis in a 2-year-old male child with Severe Acute Malnutrition (SAM) & gastroenteritis from Kalawati Saran Children’s Hospital in New Delhi.
Case Presentation
A 2-year-old male child was admitted in Paediatric Intensive Care Unit (PICU) with high-grade fever and seizures for one day. The child also had history of loose stools and vomiting on and off for the last one month. On examination, the child was in respiratory distress, encephalopathic (GCS 8/15). Patient was started on Ceftriaxone, Acyclovir, Artesunate, and Levera. The patient was electively intubated due to low GCS.
Laboratory investigations showed Hb of 7.6 gm/dl, leucocytosis (WBC: 20,100/cu mm), thrombocytopenia (platelets: 100,500/cu mm. LFT, KFT were normal. The malaria parasite was negative. CSF biochemistry & cytology were inconclusive. The CECT head was normal. Chest X-ray showed diffuse infiltrates and consolidation on the right side. Anti-TTG and HIV tests were non-reactive. The initial blood sample sent for culture was sterile. BAL culture was sterile. CSF was sterile after 48 hrs of incubation. LFA for serum galactomannan was negative. RT-PCR for H1N1 was positive. However, the condition of the patient deteriorated due to ARDS, DIC, AKI, and finally MODS, with which he succumbed by day 10.
Blood culture done on day 8 of admission, sent for blood culture done on BacT/Alert 3D (an automated colorimetric microbial detection system by Biomerieux), was positive at 11 hours of incubation. Subcultures were done on blood agar and MacConkey agar. Colonies of 2 mm–3 mm, round, non-lactose fermenting colonies were grown. The isolate Empedobacter brevis was identified by a Matrix-Assisted Laser Desorption/Ionisation-Time of Flight (MALDI-TOF) mass spectrometry system from Biomerieux. On Antibiotic Susceptibility Testing (AST), the organism was susceptible to cefepime & cotrimoxazole, intermediate to piperacillin-tazobactam & colistin, and resistant to ampicillin, amoxicillin-clavulanate, ceftazidime, cefotaxime, amikacin, gentamicin & ciprofloxacin. Epidemiological workup didn’t give any clue to the source of the origin of the microbe.
Discussion
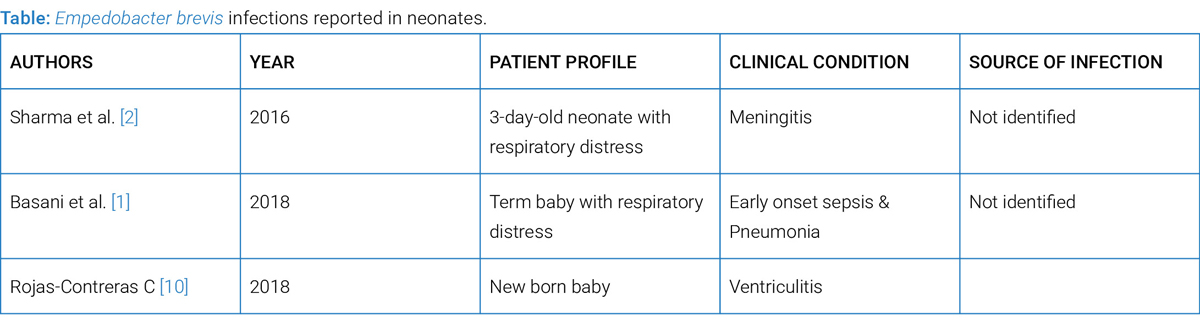
The Flavobacteriaceae family is usually yellow colony-forming bacteria which have been divided based on their genetic variation into Flavobacterium, Chryseobacterium, Myroides, and Empedobacter, with Empedobacter brevis as a distinct genetic variant [3]. E. brevis has also been found in the hospital environment, leading to many cases of nosocomial infections [6,7]. There are increasing cases of human E. brevis infections are now being reported in neonates, as showed in (Table). E. brevis, though considered rarely pathogenic, is reported to cause meningitis, pneumonia, septicaemia, and ventriculitis (Table). The bacteraemia is often associated with implanted devices, contaminated parenteral solutions, ventriculostomy drains, and vascular catheters [4,5]. E. brevis infection was reported for the first time from India in a 3-day-old neonate with sepsis and meningitis in 2016 by Sharma et al. [2].
In our case, the patient had a history of SAM and gastroenteritis for the last month. According to Bokhari et al. [8], their patient had gastrointestinal symptoms for 1 week followed by bacteraemia. Our present case is also suggestive of a strong association of gastrointestinal colonization as a source of the patient’s bacteraemia, which may have occurred during the hospital stay.
Non-Fermenting Gram-Negative Bacilli (NFGNB) cause numerous types of severe and disabling infections. There are various pathogenic organisms under the term NFGNB but the majority of serious infections are caused by Pseudomonas aeruginosa, Acinetobacter baumannii, Stenotrophomonas maltophilia and Burkholderia cepacia complex (Bcc) [9,10]. Except P. aeruginosa, the rest of the NFGNBs don’t show discernible phenotypic characteristics [11]. MALDI-TOF MS aided us in the identification of Empedobacter brevis llike non-fermenting Gram-negative bacilli (NFGNB), which are usually a challenging task using conventional methods alone.
There are no definite treatment guidelines due to the lack of validated in vitro susceptibility testing methods for this bacterium. E. brevis has been found susceptible to several classes of antibiotics, including beta-lactams, fluoroquinolones, and aminoglycosides. However, treatment of infections caused by E. brevis can be difficult because of the presence of a chromosome-encoded Ambler class B beta-lactamase, which confers decreased susceptibility to extended spectrum cephalosporins and carbapenems [12].
In conclusion, E. brevis is an emerging nosocomial pathogen that can cause serious healthcare-associated infections. There is an urgent need for epidemiological surveillance in hospitals to identify the source of this rare pathogen. Implementation of aseptic precautions by healthcare personnel and proper sterilization of equipment prevents hospital-acquired infections.
Conflict of Interest
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Informed consent was obtained for this publication.
References
- Basani L, Aepala R. Empedobacter brevis causing early onset sepsis and pneumonia in a neonate: case report and review of literature. Int J Contemp Pediatr. 2018;5(2):654–656.
- Sharma D, Patel A, Soni P, Sharma P, Gupta B. Empedobacter brevis meningitis in a neonate: a very rare case of neonatal meningitis and literature review. Case Rep Pediatr. 2016;2016:7609602.
- Vandamme P, Bernardet JF, Segers P, Kersters K, Holmes B. New perspectives in the classification of the flavobacteria: description of Chryseobacterium gen. nov., Bergeyella gen. nov., and Empedobacter nom. rev. Int J Syst Bacteriol. 1994;44:827–831.
- Janknecht P, Schneider CM, Ness T. Outbreak of Empedobacter brevis endophthalmitis after cataract extraction. Graefes Arch Clin Exp Ophthalmol. 2002;240(4):291–295.
- Nishio E. [A case of Anaphylactoid purpura suggested to Empedobacter (flavobacterium) brevis infection concerned]. Arerugi. 2010;59(5):558–561.
- Chi H, Chang KY, Chang HC, Chiu NC, Huang FY. Infections associated with indwelling ventriculostomy catheters in a teaching hospital. Int J Infecti Dis. 2010;14(3):e216–e219.
- Raman S, Shaaban H, Sensakovic JW, Perez G. An interesting case of Empedobacter brevis bacteremia after right knee cellulitis. J Glob Infect Dis. 2012;4(2):136–137.
- Bokhari S, Abbas N, Singh M, Cindrich RB, Zeana C. Empedobacter brevis Bacteremia in a patient infected with HIV: case report and review of literature. Case Rep Infect Dis. 2015;2015:813528.
- Schroeder J, O’Neal C, Jagneaux T. Practically saline. J Investig Med High Impact Case Rep. 2015;27;3(4):2324709615618980.
- Rojas-Contreras C, Cruz-Ku GD, Eyzaguirre-Sandoval ME, Valcarcel-Valdivia B. [Neonate with Ventriculitis caused by Empedobacter brevis: report of a case in Peru]. Rev Peru Med Exp Salud Publica. 2018;35(2):326–332.
- Gautam V, Sharma M, Singhal L, Kumar S, Kaur P, Tiwari R, et al. MALDI-TOF mass spectrometry: An emerging tool for unequivocal identification of non-fermenting Gram-negative bacilli. Indian J Med Res. 2017;145(5):665–672.
- Bellais S, Girlich D, Karim A, Nordmann P. EBR-1, a novel Ambler subclass B1 beta-lactamase from Empedobacter brevis. AntimicrobAgents Chemother. 2002;46(10):3223–3227.
Keywords
Bacteremia; Empedobacter brevis; Sepsis
Cite this article
Sharma A, Randhawa VS, Gupta S. Empedobacter brevis bacteremia: a rare case report from India. Clin Case Rep J. 2026;7(1):1–3.
Copyright
© 2026 Akanksha Sharma. This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY-4.0).
Copyright
.
