Abstract
This report presents a patient who developed a difficult airway during elective endotracheal intubation for general anesthesia and was subsequently diagnosed with Tracheobronchopathia Osteochondroplastica (TBPO), a rare condition. By reporting this case and reviewing the relevant domestic and international literature, we seek to improve clinical awareness of this under-recognized disease.
Abbreviations
TBPO: Tracheobronchopathia Osteochondroplastica; CT: Com¬puted tomography; GGO: Ground-glass opacity.
Introduction
Tracheobronchopathia Osteochondroplastica (TBPO) is a rare benign airway lesion of unknown etiology with no characteristic symptoms or signs. We herein report a case of TBPO diagnosed at Dujiangyan Shoujia Hospital, as presented below.
Case Presentation
A 75-year-old male was admitted to our hospital with a six-month history of recurrent epigastric pain. The pain was intermittent, localized to the epigastrium, non-radiating, and unaccompanied by nausea, vomiting, chills, fever, or diarrhea. Abdominal Color Doppler Ultrasound at a local hospital revealed cholelithiasis with cholecystitis, and the patient was subsequently admitted for elective surgical intervention.
His past medical history was significant for hypertension and type 2 diabetes mellitus for 1 year, both managed with oral pharmacotherapy (specific agents unknown). He denied a history of cardiovascular disease, infectious diseases including hepatitis, tuberculosis, typhoid fever, malaria, and dysentery, as well as a history of surgery, trauma, blood transfusion, and food or drug allergy. He had no history of smoking, alcohol consumption, or substance abuse, and no exposure to industrial toxicants, dust, or radioactive materials.
Laboratory investigations: No significant abnormalities were identified.
Chest Computed Tomography (CT):- Right middle lobe volume loss and atelectasis with tortuous, dilated bronchi, compatible with chronic infection.
- Multiple tiny solid nodules and Ground-Glass Opacities (GGOs) in both lungs, consistent with imaging features of benign nodules; annual follow-up is recommended.
- Patchy hyperdense opacity in the medial segment of the right middle lobe.
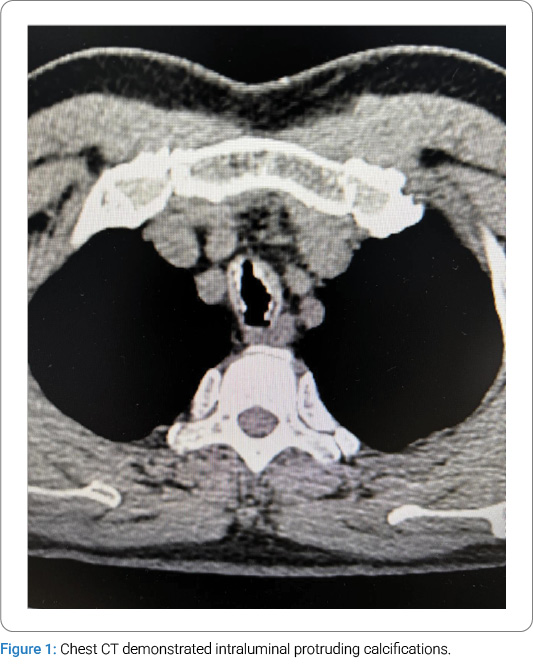
- Multiple calcifications involving the tracheal and main bronchial walls, with partial protrusion into the lumen, are suspicious for Tracheobronchopathia osteochondroplastica (TBPO) or other etiologies.
- Osteophytes of several thoracic vertebrae.
Diagnostic and Therapeutic Process:Following admission, preoperative preparations were promptly completed. On January 14, 2025, the patient was scheduled for a laparoscopic cholecystectomy under general anesthesia with endotracheal intubation. Routine anesthetic induction was administered with sufentanil 50 μg, midazolam 2 mg, etomidate 12 mg, and rocuronium 50 mg. After an adequate anesthetic effect was achieved, a video laryngoscope was inserted for endotracheal intubation, during which abnormal mucosal proliferation was noted in the trachea below the glottis (Figure 2). A senior anesthesiologist was consulted, and a visual stylet was utilized, revealing extensive proliferation distal to the glottis. A review of the chest CT demonstrated intraluminal protruding calcifications (Figure 1). Mask ventilation was maintained, and neuromuscular blockade was reversed. Following the patient’s full recovery of consciousness, the attending physician informed the patient’s family of the need for further investigations to clarify the airway pathology. The surgery was canceled, and the patient was transferred back to the ward. Subsequent flexible laryngoscopy and bronchoscopy revealed irregular exophytic lesions involving the trachea from the subglottic regionto the carina, accompanied by tracheal stenosis. Multiple scattered nodular changes were observed in the airway, with severe stenosis in the lower tracheal segment precluding bronchoscopic passage. Three biopsy specimens were obtained from the upper and middle tracheal segments and submitted for pathological examination. Pathological diagnosis: Chronic inflammatory cell infiltration of the mucosa, with squamous metaplasia and abundant calcified deposits.
Clinical diagnosis: Tracheobronchopathia osteochondroplastica (TBPO)?

Discussion
Tracheobronchopathia Osteochondroplastica (TBPO) was first identified by Rokitarisky during autopsy [1], with a male-to-female incidence ratio of approximately 3:1 [2]. Its etiology remains elusive, and there are no pathognomonic symptoms or signs. Potential etiological factors include congenital developmental anomalies of tracheobronchial cartilage [3], chronic inflammation and fibrosis of the tracheobronchial mucosa [4], and autoimmune mechanisms [5].
Three-dimensional reconstruction of chest Computed Tomography (CT) is the preferred imaging modality, as it can delineate the location and severity of stenosis [6]. Bronchoscopy serves as the gold standard for TBPO diagnosis, enabling direct visualization of the stenotic morphology and biopsy acquisition [7]. Owing to the absence of pathognomonic symptoms and signs, the condition is often undetected preoperatively. Even in the absence of typical manifestations, a detailed airway-focused medical history should be elicited. For suspected cases, three-dimensional CT of the trachea or bronchoscopy is recommended [8].
Conclusions
This case was identified during endotracheal intubation following routine anesthetic induction. The chest CT was not thoroughly reviewed during the preoperative anesthetic visit and evaluation, resulting in an unanticipated difficult airway intra-operatively. A video laryngoscope was utilized promptly, and airway abnormalities were detected without attempting blind intubation. Adequate mask ventilation was maintained throughout the process, neuromuscular blockade was reversed, and the surgery was aborted after the patient regained full consciousness, with no severe complications observed. This case highlights the importance of meticulously reviewing medical records, laboratory data, and imaging findings during preoperative anesthetic assessment to evaluate anesthetic risks comprehensively. In the setting of an unanticipated difficult airway, the paramount principles are to secure adequate ventilation, prioritize patient safety, and refrain from blind intubation attempts.
Declarations
Ethics approval and consent to participate. Not applicable.
Conflict of Interest
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Informed consent was obtained for this publication.
Keywords
Tracheobronchopathia osteochondroplastica; Computed tomography; Anesthesia
Cite this article
Zeng J. Tracheobronchopathia Osteochondroplastica Causing a Difficult Airway: A Case Report. Clin Case Rep J. 2026;7(1):1–3.
Copyright:
© 2026 Jing Zeng. This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY-4.0).
