Abstract
Spontaneous Spinal Subdural Hematoma (SSSH) is a rare presentation at the emergency department with potentially deadly outcomes. We present the case of an 80-year-old woman who presented with excruciating back pain without neurological deficits, which was later diagnosed as a thoracic SSSH. During the hospitalization, she developed Takotsubo Cardiomyopathy (TCM). Conservative treatment failed to relieve her pain, so she underwent surgery, which led to clinical improvement. This case highlights the need for clinicians to be aware of the possibility of intraspinal hemorrhages presenting without neurological deficits and how delayed diagnosis can lead to Takotsubo cardiomyopathy.
Abbreviations
SSSH: Spontaneous Spinal Subdural Hematoma;
TCM: Takotsubo cardiomyopathy;
ECG: Electrocardiogram;
bpm: Beats per Minute;
MRI: Magnetic Resonance Imaging;
TGA: Transient Global Amnesia;
IV: Intravenous;
CT: Computer Tomography;
EF: Ejection Fraction
Introduction
Spontaneous Spinal Subdural Hemorrhages (SSSH) are rare accumulations of blood in the dural space without preceding trauma and are most often associated with vascular malformations or coagulopathies (mostly due to anticoagulant use). Patients are predominantly female, frequently presenting with motor deficits and an acute onset of pain. Notably, the most common localization of the hemorrhage is the thoracic spine [1]. In rare cases, concomitant Takotsubo cardiomyopathy (TCM) has been reported in the literature, though this association remains poorly understood. It is important to note that acute neurologic diseases, such as hemorrhages, are well-established triggers for TCM [2]. Furthermore, physical stress or severe pain [3] has been described as a more common precipitant than emotional stressors [4]. In our patient, we believe that the delayed diagnosis of SSSH and severe pain led to TCM, likely induced by excessive sympathetic stimulation and catecholamine release [5,6]. Although spontaneous remission of symptoms and hematoma in SSSH has been reported [7], and conservative treatment may be considered for mild cases [8], surgical intervention with laminectomy and hematoma evacuation remains crucial for most cases [1,8].
Materials and Methods
We conducted a literature search on PubMed and Open Evidence using the keywords “spontaneous,” “subdural hematoma,” “spinal,” and TCM. As a result, we found two studies on SSSH and two case reports of concomitant SSSH and TCM. Notably, one of the studies was regarded as methodologically imprecise for classifying iatrogenic causes as non-traumatic. Furthermore, in this study, the main author contacted the patient by telephone for follow-ups after 12 months and 34 months.
Case Presentation
We present the case of an 80-year-old female admitted via ambulance to our emergency department due to acute back pain and subsequently treated in the internal medicine ward. Her medical history included arterial hypertension, a sigmoid resection 20 years prior, and small bowel ileus 5 years prior. Her daily medications were Enalapril 15 mg for hypertension and Aspirin Cardio 100 mg for a mild proximal stenosis of the celiac trunk.
Upon arrival, the patient described severe, immobilizing pain centered in the shoulder girdle and both subscapular regions. The pain radiated toward the neck and extended along the spine. She reported the onset of these symptoms while lying in bed at home. She denied any preceding trauma. Paramedics administered Intravenous (IV) Fentanyl, which partially alleviated her symptoms and allowed for hospital transport. On admission, her vital signs revealed a blood pressure of 165/90 mmHg, with no side-to-side difference, and a bradycardic pulse of 55 Beats per Minute (bpm). The patient was cold-sweating. Physical examination revealed no spinal or scapular tenderness and was otherwise unremarkable. Laboratory studies, including inflammatory markers, electrolytes, D-dimers, and a complete blood count, were within normal limits. Electrocardiogram (ECG) findings were unremarkable and showed no evidence of acute coronary syndrome.
Although the clinical presentation was consistent with aortic dissection, normal D-dimer levels led to the decision to defer Computer Tomography (CT) angiography. Neurological examination revealed no focal deficits, and reflexes were symmetric; moreover, there were no neurological “red flags” (e.g., sphincter dysfunction, motor weakness, blood pressure discrepancies) to warrant emergent spinal Magnetic Resonance Imaging (MRI). Notably, the patient exhibited retrograde amnesia of approximately three hours, beginning after Fentanyl administration. The patient’s pain improved within hours, prompting admission for observation and supportive treatment. The initial suspicion of aortic dissection was subsequently excluded due to a lack of confirmatory findings. Cardiovascular causes were considered unlikely based on a normal ECG, and spinal pathology was considered atypical in the absence of neurological deficits. The most probable diagnosis was therefore musculoskeletal in origin.
Despite persistent pain of varying severity, Rheumatological and Neurological consultations were initiated. These assessments identified possible muscular tension as the etiology of the symptoms and attributed the amnesia to Fentanyl exposure. Given the patient’s refusal of both oral and intravenous Paracetamol and Metamizole, with a preference solely for morphine, undiagnosed opioid abuse was considered. However, this consideration was not substantiated by the medical records or the primary care physician’s review.
Tizanidine was recommended. Due to the initial amnesia, neurology was consulted. No correlating pathology was found, and a Transient Global Amnesia (TGA) was considered unlikely, again attributing memory loss to the Fentanyl. On the second night, the patient’s condition changed as she experienced another acute pain flare-up, accompanied by a hypertensive crisis—likely pain-induced—and newly developed oxygenation issues, requiring 4 L/min via nasal cannula. Despite repeated administration of oral Oxycodone 5 mg, pain remained refractory. To rule out aortic dissection or pulmonary embolism, an emergency CT angiography was ordered, which excluded both. Bilateral pulmonary edema was detected, and IV Furosemide was administered. Following multiple doses of opioids, the patient was able to sleep.
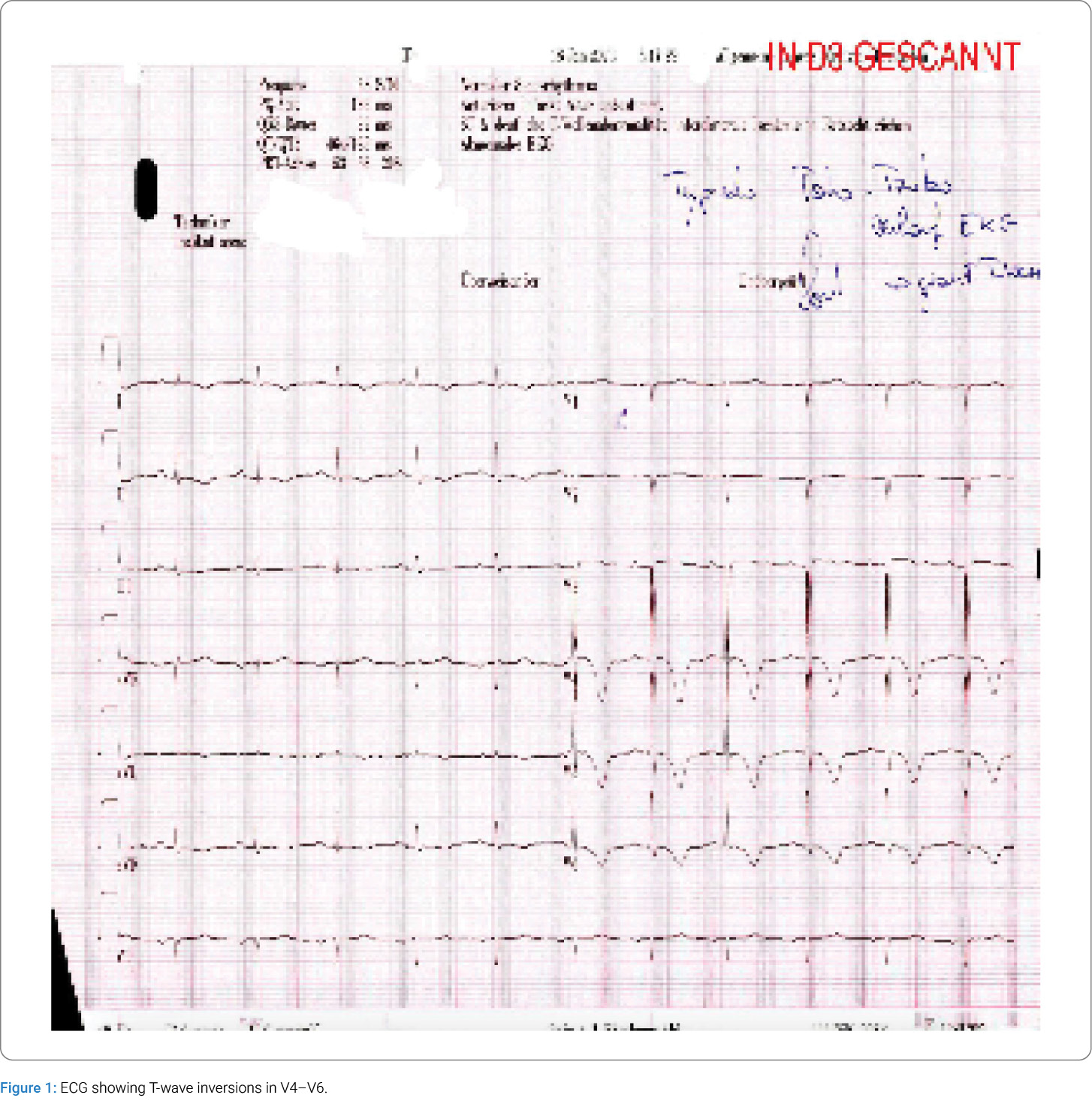
The next morning, her clinical course evolved: she reported new chest pressure. The ECG showed new T-wave inversions in leads V4–V6 (Figure 1), and the high-sensitivity troponin was elevated at 1995 ng/L. Echocardiography revealed severe hypo- to akinesia of all apical and adjacent midventricular segments, consistent with apical ballooning. Subsequently, an emergency coronary angiography revealed no stenosis, confirming the diagnosis of apical Takotsubo cardiomyopathy. Due to an initial reduced Ejection fraction (EF) of 38%, treatment was initiated with perindopril and low-dose bisoprolol. Diuretics were recommended only in case of dyspnea.
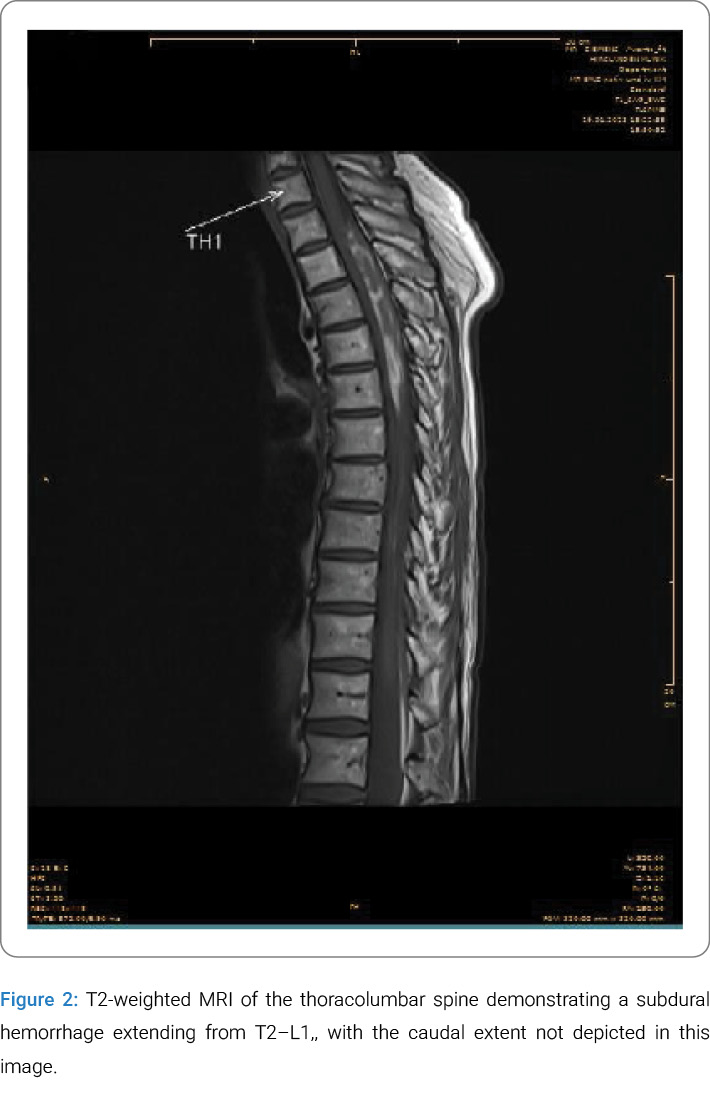
While the thoracic pain subsided, the patient’s back pain persisted without focal neurological deficits. On day 4 of her hospitalization, a spinal MRI was performed and showed a striking finding: an acute epidural and subdural intraspinal hemorrhage located dorsally, beginning at the upper plate of T2 and extending to L1. The maximal width of the hemorrhage at T4 was 8.5 mm (Figure 2). The next day, MR angiography showed no vascular abnormalities, AV fistulas, or malformations. Additionally, the patient’s brain MRI was age-appropriate and normal. These results led to the diagnosis: a rare, atraumatic, long-segment, acute-to-subacute spontaneous spinal subdural hematoma (SSSH).
Following the diagnosis, neurosurgical consultation recommended conservative treatment with analgesia and discontinuation of Aspirin Cardio (as it was no longer indicated), based on the patient’s intact neurological status and anticipated resorption of the hematoma. Despite this, comprehensive multimodal pain management was implemented; however, symptoms persisted. Over the following two weeks after admission, despite involvement of the hospital pain management team, there was no improvement. Consequently, on day 15 of hospitalization, surgical hematoma evacuation via right-sided Hemilaminectomy at T3/4, T6/7, and T9/10 was performed.
Postoperatively, the patient received Dexamethasone for two days, followed by a Ketamine infusion. During this period, she developed delirium with visual hallucinations, which were likely triggered by either the Ketamine infusion or Dexamethasone. There were no focal neurological deficits postoperatively, and her sensorimotor function remained symmetrical. However, due to the delirium and extended recovery, her hospital stay was prolonged. At discharge, her left ventricular function had improved to an EF of 51%, and her pulmonary pressures were decreasing.
She was discharged to a rehabilitation clinic on postoperative day 8. Following four weeks of rehab, she was discharged home with good pain control, having been prescribed Tapentadol, Pregabalin, Transdermal fentanyl, and Tolperisone. At this stage, she was able to walk 1 km on flat ground with two walking poles and could climb 2–3 flights of stairs. Six weeks after discharge, an MRI showed minor residual epidural and subdural scarring at T3-T5, as well as residual organizing blood at L5/S1 and in the sacral canal. One year after admission, the patient reported neuropathic thoracic pain that was controlled well with Pregabalin; however, after stopping the medication, symptoms returned. Retrospectively, she reported two months of urinary incontinence but had regained independence, resumed gardening, and no longer required walking aids. At 36-month follow-up, she showed complete remission of pain with no need for analgesics.
Discussion
Subdural spinal hematomas are most commonly associated with external trauma, followed by such iatrogenic causes as surgery or lumbar puncture. SSSH are rare and most associated with vascular malformations or coagulopathies, especially anticoagulant use [1]. Dominicucci et al. [9] conducted a literature review on SSSH in 1999, but 47% of the participant patients had received a lumbar puncture, which, in our view, should not be categorized as spontaneous. The most recent case series on SSSH from 2017 by de Beer et al. included 122 cases and reported an average age at presentation of 60 years, with a predominance of females at 57%. The thoracic spine was involved in 91% of cases, with the most common localization being thoracic alone, followed by thoracolumbar and cervicothoracic. Most patients showed motor deficits, followed by pain and sensory disturbances. Roughly half the patients were on anticoagulant drugs, and 72% required surgical decompression. A full recovery was seen in 41% of patients. These findings provide context for understanding the rarity and variability of SSSH presentations.
In light of the rarity discussed above, we identified two previously published case reports of concomitant presentation of SSSH with TCM. A case similar to ours was published in 2022 by Xiang et al. [10] of a middle-aged woman who presented with motion and sensory disturbances below the level of spinal cord compression, in addition to back pain. Sanchez et al. [11] reported a case of reverse Takotsubo likely incited by a spontaneous spinal hematoma, and a report by Ma et al. [12] described a case of acute heart failure in a young woman with global akinesia seen in her echocardiography. The cause of bleeding could not be identified in any of these cases. Interestingly, in contrast to our case, treatment was conservative and led to a good recovery, highlighting the need to treat each case individually in an interdisciplinary manner.
Our case is particularly unusual because the patient did not have neurological symptoms and was not taking oral anticoagulants. In the study by de Beer et al. [1], only 6% of patients with SSSH were receiving platelet aggregation inhibitors, as was our patient. The lack of clinical suspicion, primarily due to a normal neurological examination, contributed to a delayed diagnosis. Additionally, the severe pain likely precipitated a TCM, a rare stress-induced condition that might have been mitigated with earlier and more aggressive pain management, although the patient had declined baseline analgesia.
Our case report has several limitations. First, we observed an anchoring bias toward cardiopulmonary and later musculoskeletal pathology, most likely because the neurological examination was unremarkable. The lack of neurological symptoms was interpreted as an exclusion of spinal pathology, which might be seen as a confirmation bias. Second, the lack of early spinal imaging led to a delayed diagnosis. It was not possible to define the onset and evolution of the hemorrhage and clarify whether it contributed to the development of a TCM, which is what we suspected. Third, the cause of the hematoma remains unclear. It was not possible to establish causality between aspirin use and SSSH, or to determine whether arterial pressure fluctuations occurred before the ambulance was called, which should be treated as a possible trigger in a patient with known hypertension. Fourth, TCM comorbidity was complicated and contributed to the delay of the diagnosis of SSSH.
As with many case reports, definitive conclusions are not possible, as this case may not represent the typical course of SSSH with TCM. However, the rarity of this presentation offers valuable insight into the potential overlap and diagnostic challenges of coexisting SSSH and TCM.
Conclusion
Although a causal relationship between aspirin intake and the hematoma cannot be established, this case report emphasizes the need to critically assess ongoing pharmacotherapy and adjust it where appropriate. Furthermore, although rare, this condition demonstrates that intraspinal hematomas may occur without neurological symptoms. Based on current literature, conservative treatment is supported for mildly symptomatic cases. However, surgical decompression is often necessary—not only in those with neurological symptoms, but also in those with unbearable pain without neurological symptoms, as seen in our patient.
Acknowledgments
The authors would like to thank all clinicians and staff who contributed to the recovery of the patient, as well as the patient for consenting to the publication of this report.
Conflict of Interest
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Informed consent was obtained for this publication.
Cite this article
van Hemelrijck Meneses N, Gmür C. A Rare Case Report of Spontaneous Spinal Subdural Hematoma and Takotsubo Cardiomyopathy. Clin Case Rep J. 2026;7(2):1–5.
Copyright
© 2026 van Hemelrijck Meneses N. This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY-4.0).
