Unusual Fibrous Dysplasia with Impacted Tooth in Maxilla that Mimics Complex Odontoma
Dorsa Pourzarabi;
Mahjube Entezar-e-ghaem;
* Shahin Moeini;
-
Dorsa Pourzarabi: Department of Oral and Maxillofacial Radiology, Kashan University of Medical Sciences, Kashan, Iran
-
Mahjube Entezar-e-ghaem: Department of Oral and Maxillofacial Radiology, Shahid Sadoughi University of Medical Sciences, Yazd, Iran
-
* Shahin Moeini: Department of Oral and Maxillofacial Radiology, North Khorasan University of Medical Sciences, Bojnurd, Iran
Abstract
Background: Fibrous dysplasia (FD) is a rare, benign fibro-osseous lesion characterized by the replacement of normal bone with fibrous connective tissue and irregular trabeculae. It commonly affects the craniofacial skeleton, particularly the maxilla. While FD typically presents as a painless swelling with a characteristic “ground-glass” appearance on imaging, its association with impacted teeth, which can mimic odontogenic lesions, is uncommon.
Abbreviations: Fibrous dysplasia (FD); Cone-beam computed tomography (CBCT); Cemento-ossifying fibroma (COF)
Case Presentation: We report the case of a 16-year-old male referred with swelling in the posterior right maxilla. Clinical examination revealed facial asymmetry and intraoral expansion of the alveolar process. Radiographic evaluation, including panoramic radiography and Cone-Beam Computed Tomography (CBCT), demonstrated an expansile mixed lesion with an impacted third molar displaced toward the inferior orbital rim. The lesion exhibited classic FD characteristics, including a poorly defined border and gradual blending with normal bone. Despite mucosal thickening and discontinuity of the maxillary sinus floor, the sinus airspace remained intact, aiding in differentiation from cemento-ossifying fibroma. An incisional biopsy confirmed the diagnosis of FD based on histopathological findings.
Conclusion: This case highlights an unusual presentation of FD with an impacted maxillary third molar, resembling a complex odontoma on imaging. Accurate diagnosis requires a combination of clinical, radiographic, and histopathological assessments. Awareness of such atypical presentations is crucial for differentiating FD from other fibro-osseous and odontogenic lesions, ensuring appropriate management and surgical planning.
Introduction
Fibro-osseous lesions of the jaws comprise a group of conditions with overlapping clinical and radiographic features. FD is a benign congenital bone disorder characterized by the replacement of normal bone with fibro-osseous connective tissue, leading to an abnormal mixture of fibrous and osseous components. FD accounts for approximately 2.5% of all bone tumors [1].
FD is classified into two types: monostotic FD, which affects a single bone and represents 70%–80% of cases, and polyostotic FD, which involves multiple bones. In both forms, craniofacial involvement occurs in about half of the cases [2]. The exact etiology remains unclear, but mutations in the GNAS1 gene, which encodes a subunit of the stimulatory G protein, are believed to play a role in its pathogenesis [3].
The clinical presentation of FD varies depending on the extent of involvement. Some patients remain asymptomatic, while others present with unilateral facial swelling or progressive expansion of the alveolar process. Diagnosis is based on a combination of clinical, histopathological, and radiographic examinations [4]. Radiographically, FD typically exhibits a characteristic “ground-glass” appearance due to defective mineralization of immature dysplastic bone. The lesion has poorly defined borders with a gradual transition between dysplastic and normal bone, known as blending. Histologically, FD is characterized by curvilinear trabeculae of woven bone without osteoblastic rimming, embedded within a bland fibrous stroma devoid of malignant features [4–6].
Clinical and radiographic findings usually suffice for diagnosis. However, consulting an oral and maxillofacial radiologist and utilizing advanced imaging techniques, such as Computed tomography or CBCT, can help confirm the diagnosis and inform treatment planning. Sometimes, orthodontic or cosmetic surgery is delayed until skeletal maturation is complete [7,8].
To date, no published reports have described a case of FD involving an impacted maxillary wisdom tooth that mimicked a complex odontoma on radiographic examination. In this report, we present the clinical, radiographic, and histopathological findings of a 16-year-old male diagnosed with monostotic FD of the right maxilla, emphasizing how this case expands current knowledge.
Case Presentation
A 16-year-old male was referred to the Department of Oral and Maxillofacial Surgery, Yazd University of Medical Sciences, Iran, in 2022, presenting with swelling on the right side of the maxilla. The patient reported that the swelling had begun two years prior, with no history of systemic disease. He also had a history of tooth extraction in the affected area.
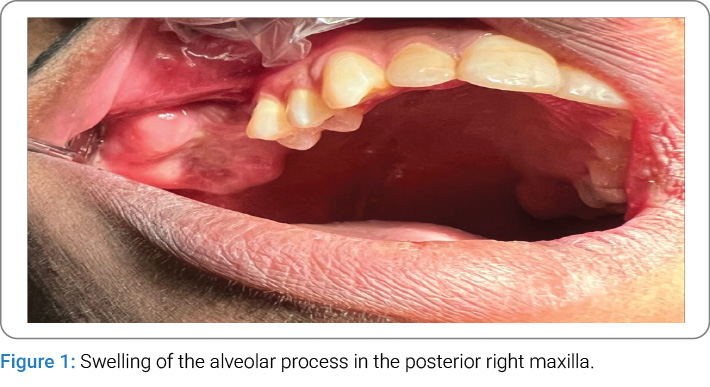
Clinical Examination: On extraoral examination, facial asymmetry was observed. Intraorally, swelling of the alveolar process in the posterior right maxilla was noted (Figure 1). The oral mucosa appeared normal without ulcerations. On palpation, the lesion exhibited a hard consistency. No lymphadenopathy, skin pigmentation, or other cutaneous abnormalities were detected. He had extracted posterior teeth because they were decayed and unrestorable.
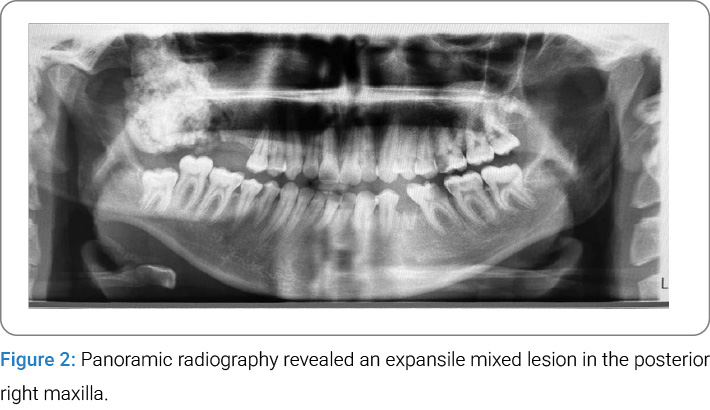
Radiographic Findings: Panoramic radiography revealed a well-defined, expansile, mixed radiolucent-radiopaque lesion in the posterior right maxilla, extending from the edentulous first molar region to the maxillary tuberosity. The lesion exhibited a non-homogeneous, cotton wool-like internal structure and partially occupied the maxillary sinus. It involved the lateral and posterolateral borders of the sinus and extended toward the pterygopalatine fissure, as evidenced by the loss of its normal anatomical definition. Vertically, the lesion extended from the alveolar crest to the level of the inferior orbital rim (Figure 2).
CBCT in cross-sectional views confirmed a non-homogeneous expansile lesion involving the right maxilla and alveolar ridge. A radiolucent rim was not observed around the lesion. The internal density resembled that of dentin or sclerotic bone, supporting its mixed radiographic appearance. The lesion caused expansion of both buccal and palatal cortical tables of the alveolar ridge with preserving overall shapes and lack of periosteal reaction (Figure 3). It was associated with an impacted third molar displaced superiorly and posteriorly toward the inferior orbital rim. In cross-sectional slice 7, narrowing of the inferior orbital fissure was evident. In slices 8 and 9, medial displacement of the lateral wall of the right posterior ethmoid air cells by the impacted tooth was identified. The lesion’s proximity to several critical anatomical structures—including the inferior orbital fissure, inferior orbital rim, and posterior ethmoid cells—is a key consideration for surgical planning (Figure 3).
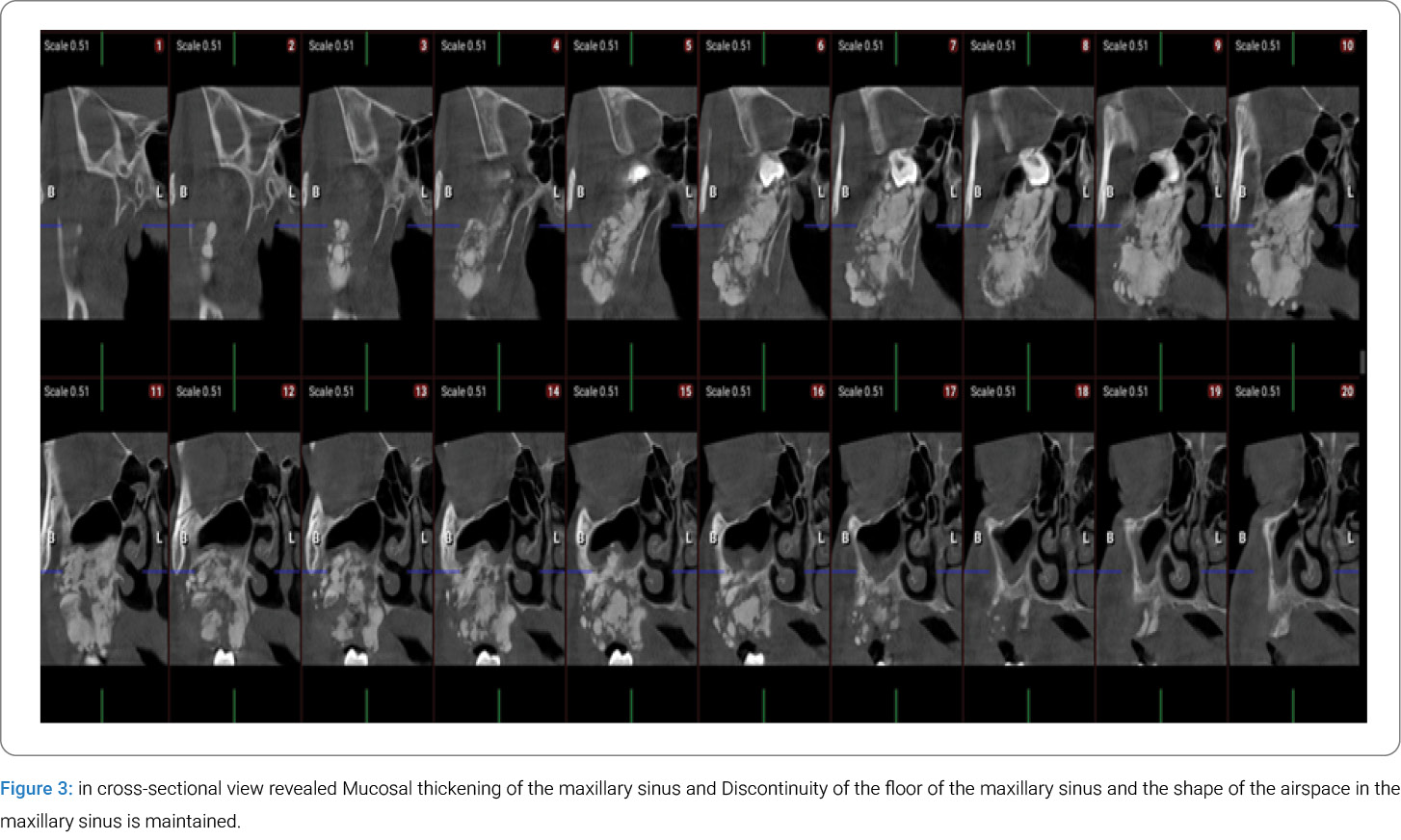
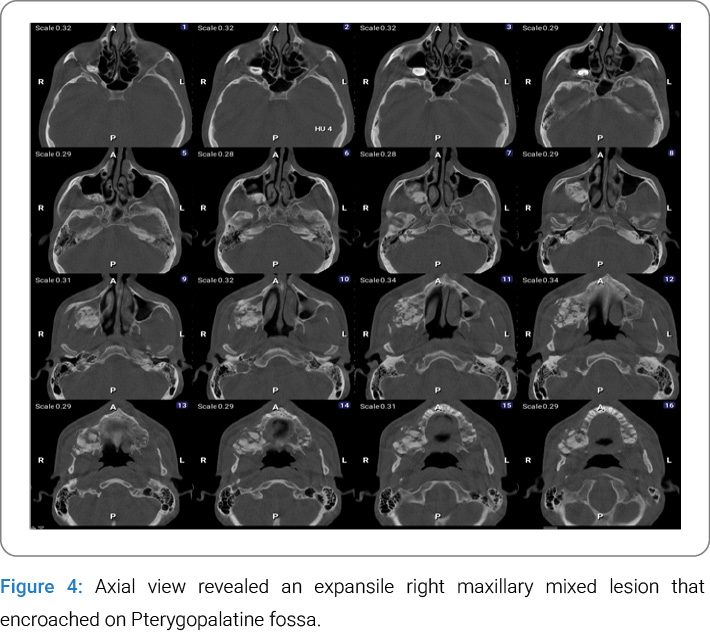
Additional CBCT findings included mucosal thickening of the maxillary sinus and disruption of its floor, as well as the anterolateral, posterolateral, and posterior sinus walls, with involvement of the osteomeatal complex (Figure 5). Axial CBCT images further demonstrated a broad and gradual transition zone between the dysplastic and adjacent normal bone, along with expansion into the pterygopalatine fossa (Figure 4). Medial displacement of the lateral wall of the nasal fossa was also observed (Figure 3).
The presence of a non-homogeneous bone pattern, an impacted tooth, involvement of adjacent critical anatomical structures, indistinct blending borders, and the lesion’s specific location all suggested multiple differential diagnoses. However, the overall preservation of the maxillary sinus airspace [9], the gradual blending of the lesion with the surrounding bone, and its anatomical location are radiographic features that strongly support a diagnosis of FD.
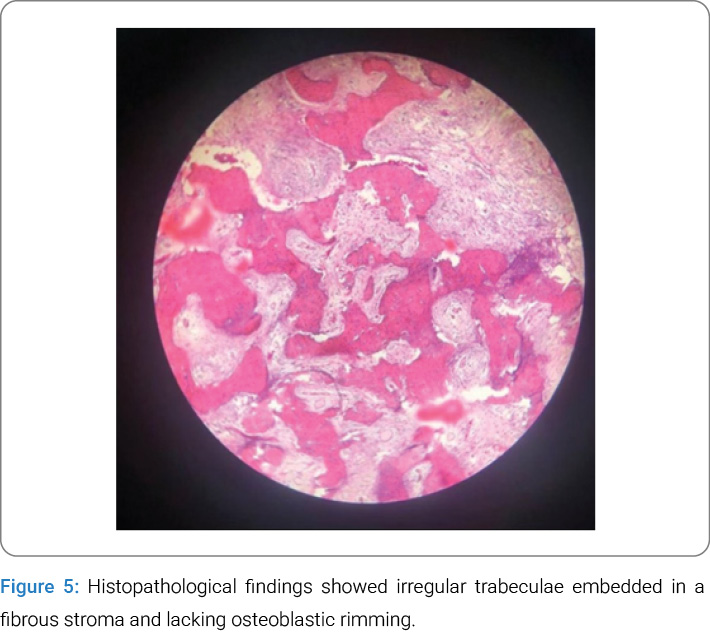
Histopathological Assessment: Based on clinical and radiographic findings, an incisional biopsy was performed. Histopathological examination confirmed the diagnosis of FD. Microscopic evaluation of the maxillary specimen revealed irregular trabeculae embedded in a fibrous stroma, lacking osteoblastic rimming, consistent with FD (Figure 5).
Treatment: The surgery involved performing an osteotomy that extended from the area of tooth #15 to the maxillary tuberosity, and vertically from the alveolar crest up to the orbital rim. The lesion was completely excised along with the impacted third molar. The excised tissue was sent for histopathological analysis to confirm the diagnosis. The area was thoroughly irrigated, and the defect was covered using a pedicle buccal fat pad flap to support healing.
Histopathology confirmed the diagnosis of FD: After surgery, the patient was prescribed antibiotics and advised to use chlorhexidine mouthwash. They were also instructed to rinse the surgical area gently with normal saline using a syringe and to stick to a soft diet to reduce irritation and help with recovery.
Discussion
The patient’s age is consistent with the typical presentation of FD, which is more common in younger individuals. While polyostotic FD usually manifests in children under 10 years of age, monostotic FD tends to present in older patients. In this case, the patient was 16-year-old, aligning with the expected age range for monostotic FD [10].
Radiographically, FD is characterized by a mixed radiolucent-radiopaque lesion with a poorly defined periphery and a gradual transition between dysplastic and normal bone, known as blending. The maxilla is the most frequently affected site [11,12]. In this case, the lesion exhibited the classic mixed appearance with a blending transition zone, located in the posterior right maxilla.
FD in the maxilla often extends into the maxillary sinus; however, an important distinguishing feature is that the shape of the sinus airspace is typically preserved [13]. In this case, mucosal thickening of the maxillary sinus and discontinuity of the sinus floor were observed, but the overall shape of the airspace remained intact. This finding is crucial for differentiating FD from COF, which often causes significant sinus obliteration [14].
Radiopaque lesions in the posterior mandible or maxilla can sometimes lead to tooth impaction, with the affected tooth being displaced either apically or coronally—a characteristic feature of complex odontomas [15,16]. However, what makes this case unique is the displacement of the impacted third molar toward the inferior orbital rim, an uncommon feature in FD.
The differential diagnosis of FD includes ossifying fibroma, Paget’s disease, osteomyelitis, and Focal Cemento-Osseous Dysplasia (FCOD). In this case, the absence of root resorption, periosteal reaction, and aggressive anatomical destruction supported the diagnosis of FD [17]. When considering a pericoronal mixed lesion, differentials such as complex odontoma, Calcifying Odontogenic Cyst (COC), and Calcifying Epithelial Odontogenic Tumor (CEOT) must be evaluated. Additionally, when assessing a mixed radiolucent-radiopaque lesion that is not necessarily associated with teeth, conditions such as COF and other fibro-osseous lesions should be considered. If malignancy is suspected, osteosarcoma and chondrosarcoma may also be included in the differential, although these are rare in such presentations.
Conclusion
The combination of clinical findings, detailed radiographic evaluation, and histopathological analysis is essential for the accurate diagnosis of fibro-osseous lesions. In this case, the use of advanced imaging—particularly CBCT—was critical in assessing the lesion’s internal structure, extent, and its relationship with adjacent anatomical landmarks, including the inferior orbital rim, posterior ethmoid air cells, and the pterygopalatine fossa. Although certain features observed—such as a cotton wool-like internal pattern, the presence of an impacted tooth, and disruption of bony boundaries—are not typically characteristic of FD and may raise suspicion for alternative diagnoses such as complex odontoma, Cemento-Ossifying Fibroma (COF), or malignancies, several key findings supported FD. The preservation of maxillary sinus contours, the lesion’s anatomical location, and its gradual transition into surrounding bone were all consistent with FD and helped narrow the diagnosis. Ultimately, histopathological analysis confirmed the diagnosis of FD. This case underscores the importance of a comprehensive diagnostic approach—particularly when lesions are located in anatomically complex regions—and demonstrates the critical role of oral and maxillofacial radiologists appropriate imaging in guiding accurate diagnosis, surgical planning, and treatment. Careful attention to characteristic radiographic features not only promotes diagnostic accuracy but also helps prevent misinterpretation and unnecessary overtreatment.
Acknowledgments
The authors would like to appreciate the continued support of the surgeon of Yazd University of Medical Science, Yazd, Iran.
References
- Ahmad M, Gaalaas L. Fibro-osseous and other lesions of bone in the jaws. Radiol Clin North Am. 2018;56(1):91–104.
- Valentini V, Cassoni A, Marianetti TM, Terenzi V, Fadda MT, Iannetti G. Craniomaxillofacial fibrous dysplasia: conservative treatment or radical surgery? A retrospective study on 68 patients. Plast Reconstr Surg. 2009;123(2):653–660.
- Yang HY, Su BC, Hwang MJ, Lee YP. Fibrous dysplasia of the anterior mandible: A rare case report. Tzu Chi Med J. 2018;30(3):185–187.
- Pinto MD, Braz G, Santos RG, Polido D, Paixão JR, de Melo SH. Fibrous dysplasia in maxillary bone: case report. Int J Oral Dent Health 2018;4(2):072.
- Burke AB, Collins MT, Boyce AM. Fibrous dysplasia of bone: craniofacial and dental implications. Oral Dis. 2017;23(6):697– 708.
- Lietman SA, Levine MA. Fibrous dysplasia. Int J Surg Pathol. 2013;10(Suppl 2):389–396.
- Hong I, Kang DC, Leem DH, Baek JA, Ko SO. An unusual presentation of non-specific cystic degeneration of craniofacial fibrous dysplasia: a case report and review of literature. Maxillofac Plast Reconstr Surg. 2020;42(1):31.
- Boyce AM, Chong WH, Yao J, Gafni RI, Kelly MH, Chamberlain CE, et al. Denosumab treatment for fibrous dysplasia. J Bone Miner Res. 2012;27(7):1462–1470.
- Shi LL, Xiong P, Zhen HT. Management strategies of fibrous dysplasia involving the paranasal sinus and the adjacent skull base. Ear Nose Throat J. 2025;104(2):85–92.
- Feller L, Wood N, Khammissa RAG,, Lemmer J, Raubenheimer EJ. The nature of fibrous dysplasia. Head Face Med. 2009;5:22.
- Lee JS, FitzGibbon EJ, Chen YR, Kim HJ, Lustig LR, Akintoye SO, et al. Clinical guidelines for the management of craniofacial fibrous dysplasia. Orphanet J Rare Dis. 2012;7 Suppl 1(Suppl 1):S2.
- Dua N, Singla N, Arora S, Garg S. Fibrous dysplasia of maxilla: report of two cases. J Indian Acad Oral Med Radiol. 2015;27:472–475.
- Whyte A, Boeddinghaus R. The maxillary sinus: physiology, development and imaging anatomy. Dentomaxillofac Radiol. 2019;48(8):20190205.
- Tompodung LM, Sensusiati AD. Ossifying fibroma of the maxilla: A case report with literature review. Radiol Case Rep. 2023;19(3):915–921.
- Shetty RM, Halawar S, Reddy H, Rath S, Shetty S, Deoghare A. Complex odontome associated with maxillary impacted permanent central incisor: a case report. Int J Clin Pediatr Dent. 2013;6(1):58–61.
- Pillai A, Moghe S, Gupta MK, Pathak A. A complex odontoma of the anterior maxilla associated with an erupting canine. BMJ Case Rep. 2013;2013:bcr2013200684
- Kochanowski NE, Badry MS, Abdelkarim AZ, Lozanoff S, Syed AZ. Radiographic diagnosis of fibrous dysplasia in maxilla. Cureus. 2018;10(8):e3127.
Keywords
Fibrous dysplasia; Maxilla; Cone-beam computed tomography; Impacted tooth; Fibro-osseous lesion
Cite this article
Pourzarabi D, Entezar-e-ghaem M, Moeini S. Unusual Fibrous Dysplasia with impacted tooth in maxilla that mimics Complex odontoma. Clin Case Rep J. 2026;7(2):1–5.
Copyright
© 2026 Shahin Moeini. This is an open access arti¬cle distributed under the terms of the Creative Commons Attri¬bution 4.0 International License (CC BY-4.0).
