Clival Mucopyocele: A Case Report and Review of the Literature
* Kianoush Sheykholeslami;
Shahil Patel;
Amin Ahmadi Nejad Masouleh;
Yura Hirota Sheykholeslami;
Simon Hanft;
-
* Kianoush Sheykholeslami: Section Otolaryngology-Head and Neck Surgery, Department of Surgery, Saint Peters University Hospital, New Brunswick, NJ, USA
-
Shahil Patel: School of Biomedical and Health Science, Rutgers University, New Brunswick, NJ, USA
-
Amin Ahmadi Nejad Masouleh: School of Biomedical and Health Science, Rutgers University, New Brunswick, NJ, USA
-
Yura Hirota Sheykholeslami: School of Biomedical and Health Science, Rutgers University, New Brunswick, NJ, USA
-
Simon Hanft: Department of Neurosurgery, Westchester Medical Center, New York Medical College, NY, USA
Abstract
Clival masses typically present as chordomas. However, this report presents a rare case of a clival mucopyocele, a benign paranasal sinus mucocele. The patient, who presented with headaches and diplopia, was later successfully treated with a trans-nasal trans-sphenoidal endoscopic approach along with a postoperative antibiotic regimen. This case report highlights the importance of comprehensive clinical and imaging evaluation, as well as the consideration of rare differential diagnoses.
Introduction
The clivus represents an enigma to most surgeons due to its intricate and highly complex location at the fusion of the occipital and sphenoid bones. This creates challenges as the location hinders clear diagnostic imaging and easy surgical access [1]. While lesions confined to the clivus may remain asymptomatic and cause little to no clinical manifestation, more aggressive lesions may cause neurological symptoms. This not only includes headaches, but also cranial nerve symptoms, including diplopia, often resulting from paralysis of the abducens nerve, which is in close proximity to the clivus. Clival masses are rare pathologic entities with chordomas representing the most frequent tumors of this region, accounting for about 40% of all cases [2]. Here, we report a case of a mucopyocele in the anterior clivus, a pathology so uncommon that only very few similar cases have been previously reported in the scientific literature [3,4]. Mucoceles are typically benign, fluid-filled cystic lesions and are very common in the paranasal sinuses. They rarely extend to surrounding structures (such as the clivus) and even more rarely present as an isolated lesion within the skull base. This case represents a deviation from the norm, which overall highlights the potential for mucoceles to occur in locations far beyond their common sites of origin. Moreover, the presence of a suprainfection in a clival mucocele has not been reported in the literature, which adds an additional layer of complexity and clinical interest.
Case Presentation
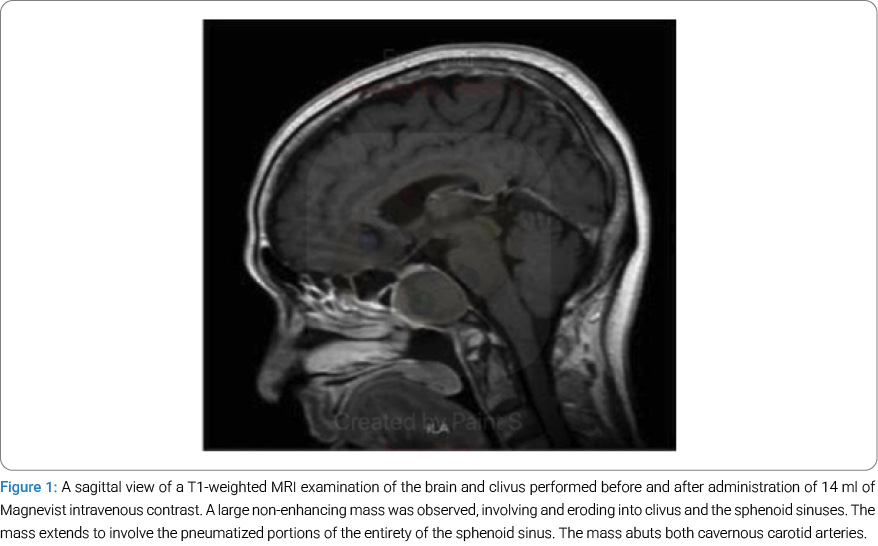
The patient is a 61-year-old Asian female who presented with progressively worsening headaches over the past 2 months, along with new-onset diplopia due to left cranial nerve IV palsy. On admission, a Computed Tomographic (CT) scan and Magnetic Resonance Imaging (MRI) were performed, revealing a 3-centimeter, well-defined, non-enhancing mass centered on and eroding into the clivus (Figure 1). A preliminary diagnosis of clival chordoma was made, and the patient underwent endoscopic endonasal trans-sphenoidal resection of the mass for diagnostic and therapeutic purposes.
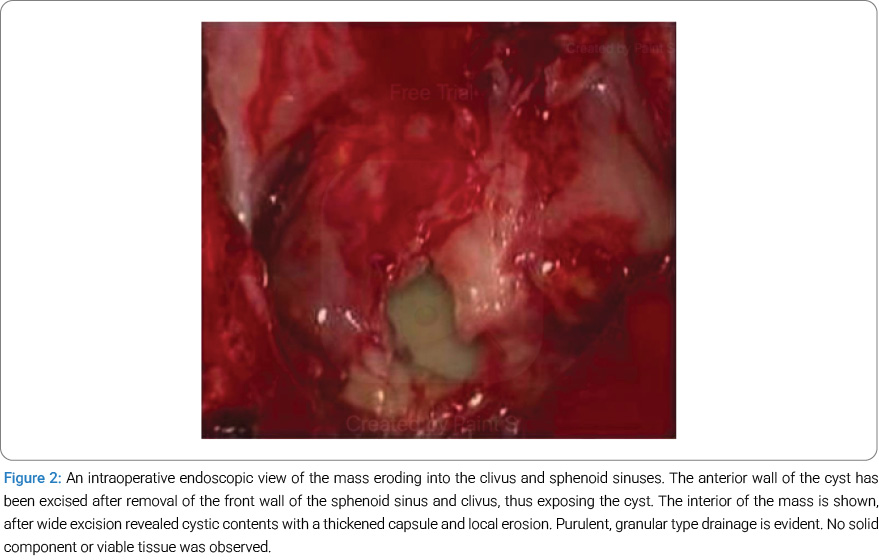
During surgery, adequate exposure was achieved through an endoscopic, endonasal trans-sphenoidal approach. The mass was identified sitting on the floor of the sphenoid sinus, replacing the clivus. The exposure was extended, and a cruciate incision was made to open the mass capsule. Upon incision, a combination of purulent and granular material was encountered (Figure 2). Using a microdebrider, the anterior wall of the mass was carefully removed and widely marsupialized. An absorbable stent was inserted into the area and left in place to maintain patency of the drainage passage during the healing process.
Interestingly, subsequent CT scans of the chest and abdomen revealed miliary pulmonary nodules that tested positive for acid-fast bacilli. The patient was subsequently started on a three-drug treatment for tuberculosis infection based on chest CT findings and culture-positive tuberculosis in the lung. The patient was not found to have any underlying immunocompromised status.
Postoperatively, pathological studies of the clival mass did not show any evidence of malignancy. Histology revealed a histiocyte-rich inflammatory lesion with small foci of necrosis and rare giant cells, favoring an infectious etiology. Subsequent cultures of the purulent fluid grew Enterobacter aerogenes, but were negative for acid-fast bacilli. The patient was treated with intravenous ceftriaxone postoperatively, with resolution of both her headaches and diplopia.
Differential Diagnosis: Bony erosion is extremely rare for notochordal remnants. When it occurs with restricted diffusion, it should raise suspicion for clival chordoma. Clival chordoma is considered the malignant counterpart of ecchordrosis and its primary mimicker. In our case, bony erosion with restricted diffusion on MRI initially raised concern for chordoma, a malignant notochordal remnant. Other differential diagnoses included dermoid cysts, arachnoid cysts, sphenoid sinus cysts or herniations, petroclival meningiomas, metastatic lesions, and benign entities like neurenteric cysts, hemangiomas, arrested pneumatization, and fibrous dysplasia. Radiologic features were critical in narrowing the differential. The final diagnosis required surgical exploration and histopathologic confirmation.
Discussion
The clivus can be affected by different congenital or acquired pathologies, including tumors, inflammatory conditions, and infectious processes. The most common clival tumors are chordomas and chondrosarcomas, both of which have a relatively high incidence in this area. A clival mucopyocele is an extremely rare entity, and its exact pathogenesis is unknown. Previous case reports have not clearly identified causes of this lesion, but speculate that developmental abnormalities allowing for clivus pneumatization and subsequent communication with the sphenoid sinus may allow mucocele formation upon obstruction of this communication [3]. A similar pathogenesis may have led to the formation of the mucocele in our patient, which was secondarily infected through hematogenous seeding from a primary respiratory process or via direct inoculation from the sphenoid sinus.
Diagnostic imaging plays a central role in surgical planning and the accurate diagnosis of inflammatory and neoplastic lesions of the clivus. Here, we describe a few common pathologies involving the clivus from a radiologic standpoint. On CT, chordomas appear as centrally located, expansile soft-tissue masses arising from the clivus, often with extensive bone destruction and intratumoral calcifications. On MRI, they are hypointense on T1 and very hyperintense on T2-weighted images, which is a characteristic finding. Chondrosarcomas appear as well-defined osteolytic lesions with a characteristic ring and arc calcifications on CT. They are iso- to hypointense on non-contrast T1-weighted images and hyperintense on T2-weighted MRI, with intense heterogeneous enhancement.
In contrast to chordomas, chondrosarcomas are off midline. Mucoceles of the sphenoid sinus are locally expansile lesions with thinning and erosions of sinus walls, and they can erode intracranially to involve the clivus. Signal characteristics on MRI depend on the content of the lesion. When rich in protein, the lesion appears homogeneously hyperintense on T1- and T2-weighted sequences with no post-contrast enhancement. Clival involvement by fibrous dysplasia is extremely rare and would typically present as a sclerotic lesion, where the inner table becomes thickened. Ground-glass density, ballooning, and expansion of the affected bone and thinning of the cortex are the hallmarks of fibrous dysplasia. MRI reveals a hypointense lesion on T1-weighted images and a variable (usually low) signal intensity lesion on T2-weighted images, with heterogeneous post-contrast enhancement. Meningiomas, the most common benign intracranial neoplasms in adults, are hyperdense on non-contrast-enhanced CT and show homogeneous enhancement on post-contrast imaging.
They are hypo- to isointense on T1- and T2-weighted sequences, with intense homogenous enhancement and a characteristic dural tail. Langerhans cell histiocytosis is a rare but possible cause of a clival mass in the pediatric population. It typically presents as destructive, lytic bone lesions with a characteristic ‘punched out’ appearance [6]. On MRI, the lesions are hyperintense on T2 and hypointense on T1-weighted images with homogeneous or heterogeneous enhancement of the destructive soft tissue mass and variable local extension. Diffusion restriction may be seen due to the increased cellularity. Once clival Langerhans Cell Histiocytosis is detected, it is important to evaluate for synchronous lytic lesions in other areas of the skeleton. Aneurysmal bone cysts are well-differentiated benign osteolytic tumors commonly seen in individuals under 20 years of age. Plain radiographs usually show a complex cystic lesion, while erosion and thinning of the cortex are better seen on CT. MRI shows classical multiple fluid levels and internal septations, indicative of hemorrhage with sedimentation [6].
The primary therapy for all clival masses is surgery [5]. The complex anatomy of this region makes surgical access difficult. We used an endoscopic trans-nasal trans-sphenoidal approach to isolate the clivus, providing adequate visualization of anatomical structures while limiting the need for extensive exposure that could compromise nearby structures such as the carotid arteries or cranial nerves [4]. Image guidance is essential for determining the exact location and boundaries of the lesion in order for adequate resection [7].
Conclusion
Although clival masses are rare, chordomas remain the most frequently encountered tumors in this region, among other pathologies that can be seen. This case report highlights a mucopyocele in the clivus that initially presented as a chordoma. Therefore, multidisciplinary cooperation among radiologists, pathologists, neurosurgeons, and otolaryngologists is essential. However, only through direct visualization during surgery and follow-up laboratory studies was the true nature of the lesion accurately identified. Thus, it is imperative to maintain a wide differential diagnosis when approaching a clival mass, as chordomas are not the only lesions that can occur in this area.
Summary
- Correct diagnosis of clival pathology is crucial for proper treatment.
- This case report discusses a new, rare diagnosis and treatment for a clival mass.
Patient consent statement
Written informed consent was obtained from the patient for the publication of this case report.
Ethics Statement
As a single-case report with the patient’s signed consent, no other ethical review was required.
Acknowledgement
Shahil Patel: Manuscript writing, study format deign, data curating, investigation.
Yura Hirota Sheykholeslami: Literature review, data gathering, investigation.
Amin Ahmadi Nejad Masouleh: Literature review, data gathering, investigation.
Kianoush Sheykholeslami: Study Design, project administration, obtaining permissions, investigation, methodology, validation, manuscript writing, supervision, data curation, reviewing and editing.
Conflicts of Interest
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Informed consent was obtained for this publication.
References
- Leonetti JP, Reichman OH, Al-Mefty O, Li J, Smith PG. Neu¬rotologic considerations in the treatment of advanced clival tumors. Otolaryngol Head Neck Surg. 1992;107(1):49–56.
- Filippo G, Spina A, Boari N, Narayanan A, Mortini P. Solitary Lesions of the Clivus: What Else besides Chordomas? An Extensive Clinical Outlook on Rare Pathologies. Acta Neurochir (Wien). 2015;157(4):597–605; discussion 605.
- Yasunori F, Harada Y, Toyota S, Wakayama A, So H, Yoshimine T. Primary clival mucocele: case report. Neurol Med Chir (Tokyo). 2011;51(3):250–252.
- Stavrakas M, Khalil HS, Tsetsos N, Muquit S. Clival mucocele: A rare yet not forgotten pathology. Ear Nose Throat J. 2023,102(10):632–634.
- Fernandez-Miranda JC, Gardner PA, Snyderman CH, Devaney KO, Mendenhall WM, Suárez C, et al. Clival chordomas: A pathological, surgical, and radiotherapeutic review. Head Neck. 2014;36(6):892–906.
- Gomez CK, Schiffman SR, Bhatt AA. Radiological review of skull lesions. Insights Imaging. 2018;9(5):857–882.
- González-García L, Asenjo-García B, Bautista-Ojeda MD, Domínguez-Páez M, Romero-Moreno L, Martín-Gallego A, et al. Endoscopic endonasal resection of clival xanthoma: case report and literature review. Neurosurg Rev. 2015;38(4):765– 769.
Cite this article
Patel S, Masouleh AAN, Sheykholeslami YH, Hanft S, Sheykholeslami K. Clival Mucopyocele: A Case Report and Review of the Literature. Clin Case Rep J. 2026;7(2):1–4.
Keywords
Clival mucopyocele; Chordomas; Clival mass
Copyright
© 2026 Kianoush Sheykholeslami. This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY-4.0).
