Squamous Metaplasia of the Lactiferous Ducts: An Underrecognized Manifestation of Hidradenitis Suppurativa? A Case Report
* Vera Santis GA;
Klinger Guerra RG;
Garate González ME;
Morales Huber CM;
Carreño Toro LE;
Whittle Pinto CI;
-
* Vera Santis GA: Department of Dermatology, University of Chile, Santiago, Chile
-
Klinger Guerra RG: Department of Dermatology, University of Chile, Santiago, Chile
-
Garate González ME: Department of Dermatology, University of Chile, Santiago, Chile
-
Morales Huber CM: Department of Pathology, University of Chile Clinical Hospital, Santiago, Chile
-
Carreño Toro LE: Department of Pathology, University of Chile Clinical Hospital, Santiago, Chile
-
Whittle Pinto CI: Department of Radiology, Alemana Clinic, Santiago, Chile
Abstract
Squamous Metaplasia of Lactiferous Ducts (SMOLD), previously known as Zuska’s disease, is a rare inflammatory breast disorder characterized by recurrent subareolar abscesses and chronic mammary fistula formation, typically occurring in non-lactating women. It accounts for approximately 1%–2% of symptomatic Breast diseases and is frequently underdiagnosed due to low clinical suspicion, which may lead to unnecessary treatments and delayed appropriate management. Although originally described as a distinct form of non-puerperal mastitis, current hypotheses suggest a possible association with Hidradenitis Suppurativa (HS), as both conditions share similar clinical and pathophysiological features.
We present the case of a 50-year-old female smoker who initially developed left submammary inflammatory nodules consistent with HS. She subsequently presented with right periareolar skin involvement, which was treated with multiple antibiotic regimens for presumed infectious mastitis. The lesions later progressed into three erosive plaques. Ultrasound demonstrated an intradermal collection with a hypoechoic linear tract suggestive of a fistula; histopathological examination revealed chronic dermatitis, ductal ectasia, and a mixed inflammatory infiltrate. Special stains for infectious organisms were negative. Based on the clinical, radiological, and pathological findings, a diagnosis of SMOLD disease was established. The patient demonstrated a good clinical response to lymecycline and intralesional corticosteroids.
This case emphasizes the clinical and pathological overlap between SMOLD and HS. The coexistence of chronic mammary fistulae and HS lesions in the same patient supports the hypothesis that SMOLD may represent a localized manifestation within the hidradenitis spectrum. Recognizing this association is crucial to avoid misdiagnosis, minimize unnecessary treatments, and enable early intervention for improved patient outcomes.
Abbreviations
SMOLD: Squamous Metaplasia of Lactiferous Ducts
HS: Hidradenitis Suppurativa
Introduction
Squamous Metaplasia of Lactiferous Ducts (SMOLD), previously known as Zuska’s disease [1], is characterized by one or more recurrent subareolar breast abscesses secondary to ductal obstruction, occurring in non-lactating, non-postpartum women [2]. This condition follows a clinical course similar to that of Hidradenitis Suppurativa (HS), with recurrent inflammatory flares and persistent fistula formation. This underdiagnosed entity is frequently overlooked due to low clinical suspicion, resulting in delayed treatment, increased patient morbidity, and impaired quality of life [3].
Case Presentation
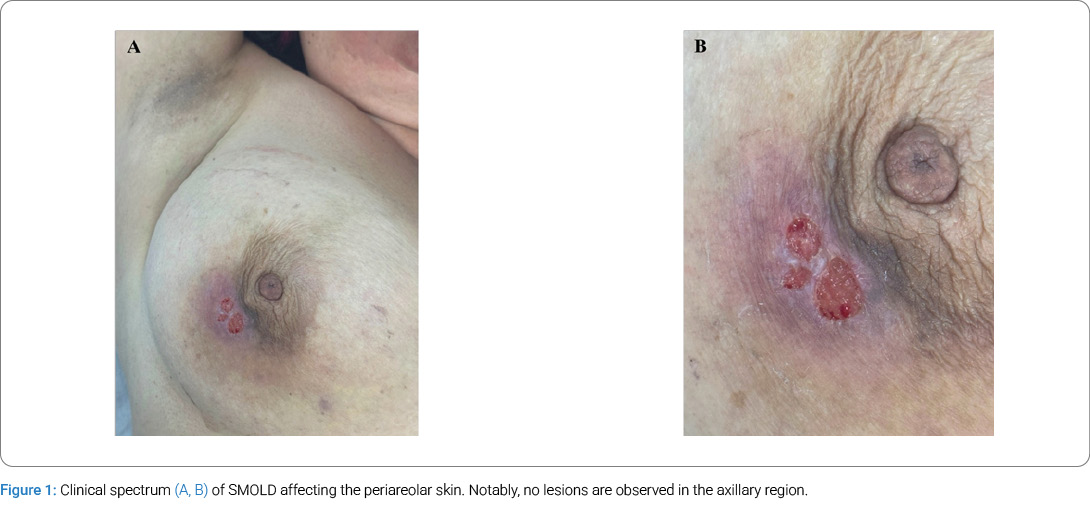
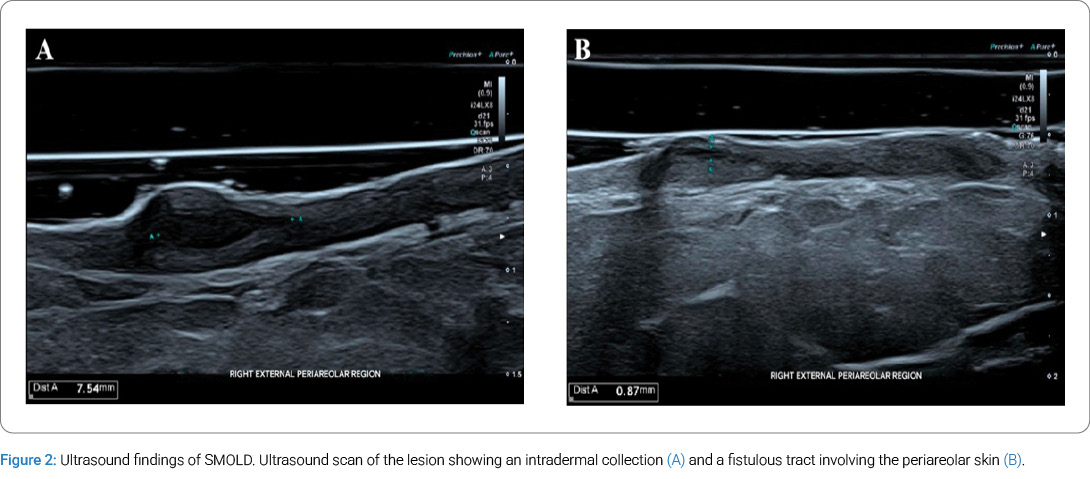
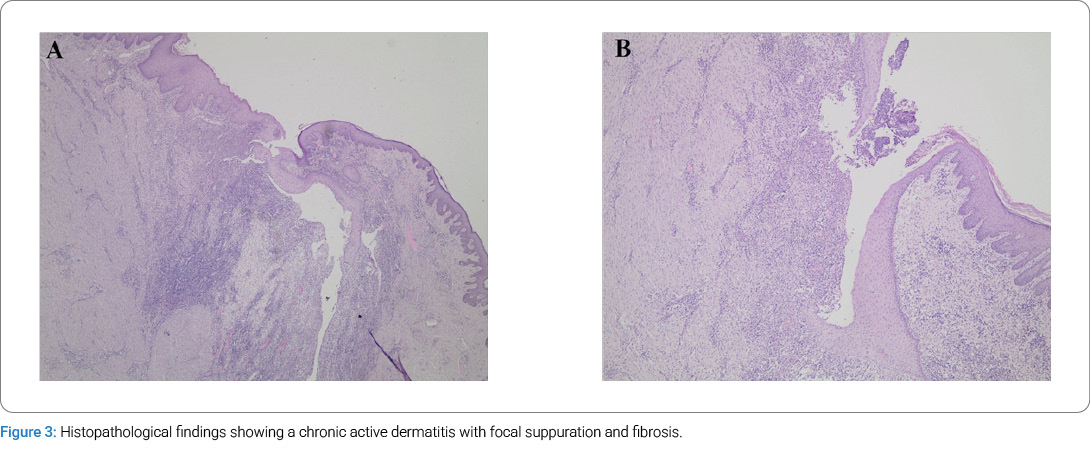
We present the case of a 50-year-old female smoker with scarring in the axillary and inguinal regions, along with an inflammatory nodule in the left submammary area. She was treated with oral doxycycline combined with topical treatment, resulting in a variable response. Subsequently, the patient developed a painful, indurated erythema affecting the periareolar skin of the right breast. Multiple antibiotic regimens were prescribed for presumed infectious mastitis. Eventually, the lesion progressed to three erosive plaques with an erythematous-violaceous appearance and granulation tissue (Figure 1A, Figure 1B). Ultrasound revealed marked dermal thickening, hypervascular inflammatory tissue, and a 7.5 mm × 1.8 mm intradermal collection with a hypoechoic linear band consistent with a fistulous tract (Figure 2A, Figure 2B). The ultrasound report suggested considering SMOLD as the primary diagnosis. Histopathology (Figure 3A, Figure 3B) showed chronic dermatitis with fibrosis and a mixed inflammatory infiltrate, along with a focal fistulous tract. Ductal ectasia and lymphocytic periductitis were also observed. PAS, Gram, and Ziehl-Neelsen stains were negative. No evidence of malignancy was identified. Based on clinical, ultrasonographic, and histopathological findings, a diagnosis of SMOLD was established. The patient was subsequently treated with lymecycline and intralesional corticosteroid, with a clinical improvement.
Discussion
This entity was first described in 1951 by Zuska, who detailed the clinical and pathological features of five women presenting with a distinctive form of non-puerperal mastitis [4]. It accounts for approximately 1%–2% of symptomatic breast disorders [5], with a median age of presentation at 47 years [4,6]. It is considerably more common in women; in contrast, this disease in men is exceedingly rare, with fewer than 20 cases reported [7]. The condition is clinically defined by a triad: a subareolar fistulous tract, persistent nipple discharge, and recurrent, multifocal breast abscesses. As reported in a retrospective study conducted by Fu et al., 25%–40% of patients with this condition develop recurrent abscesses, and 33% develop cutaneous fistula formation [8].
These findings are most frequently observed in women with a history of smoking, attributed to squamous metaplasia of the ductal epithelium of the lactiferous ducts [9]. The risk of developing a primary breast abscess is six times higher in smokers, who are also fifteen times more likely to experience recurrence [1]. Additional risk factors for squamous metaplasia include trauma, diabetes mellitus, iatrogenic procedures, immunosuppression, and nipple piercing [2]. The differential diagnosis should include other conditions located in the subareolar region, such as acute mastitis, infected sebaceous cysts, infections of the Montgomery tubercles, or malignancy.
SMOLD shares clinical characteristics and likely pathophysiological mechanisms with HS, presenting a chronic, recurrent course marked by episodes of inflammatory activity and fistula formation. Both conditions predominantly affect women between 20 and 50 years of age, show a strong association with smoking, and significantly impair quality of life. Therapeutic approaches are also comparable, typically involving antibiotics, anti-inflammatory agents, and surgical intervention. The coexistence of chronic breast fistula and HS in the same patient supports the hypothesis that SMOLD may represent a localized manifestation within the hidradenitis spectrum [9]. A complete excision of the fistula and the abnormal duct is recommended to prevent recurrent episodes, especially since cases of primary squamous cell carcinoma of the breast have been reported in association with SMOLD [10], along with smoking cessation, which is essential.
Conclusions
SMOLD is an uncommon, under-recognized entity that should be considered in the differential diagnosis of chronic periareolar inflammation, especially in patients with coexisting HS or relevant risk factors such as smoking. Its clinical and pathological overlap with HS suggests a possible shared inflammatory pathway. Dermatologists must maintain a high index of suspicion to avoid misdiagnosis, minimize unnecessary treatments, and enable early intervention for improved patient outcomes. Definitive treatment of SMOLD requires formal surgical excision.
Conflict of Interest
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Informed consent was obtained for this publication.
References
- Ofri A, Dona E, O’Toole S. Squamous metaplasia of lactiferous ducts (SMOLD): an under-recognised entity. BMJ Case Rep. 2020;13(12):e237568.
- Gollapalli V, Liao J, Dudakovic A, Sugg SL, Scott-Conner CEH, Weigel RJ. Risk factors for development and recurrence of primary breast abscesses. J Am Coll Surg. 2010;211(1):41–48.
- Hanavadi S, Pereira G, Mansel RE. How mammillary fistulas should be managed. Breast J. 2005;11(4):254–256.
- Zuska JJ, Crile G Jr, Ayres WW. Fistulas of lactifierous ducts. Am J Surg. 1951;81(3):312–317.
- Dixon JM. Periductal mastitis/duct ectasia. World J Surg. 1989;13(6):715–720.
- Livingston SF, Arlen M. Ductal fistula of the breast. Ann Surg. 1962;155(2):316–319.
- Gkionis IG, Giakoumakis MI, Liva D, Tsioulos G, Matalliotakis M, Vrontaki M, et al. Zuska’s disease in a male patient. The critical role of ultrasound imaging in diagnosis and management of this rare entity. Radiol Case Rep. 2023;18(6):2149–2153.
- Fu P, Kurihara Y, Kanemaki Y, Okamoto K, Nakajima Y, Fukuda M, et al. High-resolution MRI in detecting subareolar breast abscess. AJR Am J Roentgenol. 2007;188(6):1568–1572.
- Cosman BC, Al-Refaie WBH. Mammillary fistula as a manifestation of acne inversa (hidradenitis suppurativa): report of two cases. J Am Coll Surg. 2002;194(6):829–833.
- Huws AM, Semkin L, Moalla A, Udayasankar S, Holt SDH, Sharaiha YM. Primary squamous cell carcinoma of the breast in association with Zuska’s disease. Breast Cancer. 2018;25(3):365–369.
Cite this article
Vera Santis GA, Klinger Guerra RG, Garate González ME, Morales Huber CM, Carreño Toro LE, Whittle Pinto CI. Squamous Metaplasia of the Lactiferous Ducts: An Underrecognized Manifestation of Hidradenitis Suppurativa? A Case Report. ClinCase Rep J. 2026;7(2):1–4.
Keywords
Zuska disease; Fistula; Breast disease; Abscess
Copyright
© 2026 Vera Santis GA. This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY-4.0).
