Hypercalcemia due to Vitamin D Toxicity and Acute Kidney Injury: Clinical Case and Review
* Spivacow Francisco;
Robaina Javier;
del Valle Elisa;
Albertón Valeria;
-
* Spivacow Francisco: Instituto de Investigaciones Metabólicas, Universidad del Salvador, Buenos Aires, Argentina
-
Robaina Javier: Division of Nephrology, Hospital de Clínicas, University of Buenos Aires, Buenos Aires, Argentina
-
del Valle Elisa: Instituto de Investigaciones Metabólicas, Universidad del Salvador, Buenos Aires, Argentina
-
Albertón Valeria: Servicio de Anatomía Patológica, Hospital Fernández and Hospital El Cruce, Buenos Aires, Argentina
Abstract
A 35-year-old patient with no significant medical history presented with acute kidney injury. A renal biopsy revealed acute tubular necrosis. The kidney injury was due to hypercalcemia caused by iatrogenic vitamin D toxicity. The case resolved with fluid and electrolyte replacement and furosemide. A review of the topic follows.
Introduction
Growing evidence suggests that maintaining adequate 25-hydroxyvitamin D [25(OH)D] levels is essential for preventing various chronic diseases [1–6]. Vitamin D is a fat-soluble vitamin. It is obtained through dietary sources, including animal products and fortified foods, or by endogenous synthesis [7]. Furthermore, it is widely available as both a prescription and an over-the-counter supplement.
Although vitamin D deficiency is prevalent worldwide, excessive intake leading to toxicity is rare but potentially life-threatening. However, vitamin D intoxication can induce severe hypercalcemia, which in turn can cause significant complications, including Acute Kidney Injury (AKI), cardiac arrhythmias, and neurological impairment [8].
The pathophysiology of hypercalcemia in this context involves both enhanced intestinal calcium absorption and increased bone resorption [9]. These effects are mediated by markedly elevated 25(OH)D levels. High levels may directly activate the vitamin D receptor or displace other active metabolites from their binding proteins. This increases the free concentrations of these metabolites [10,11].
Despite its clinical significance, reports of AKI secondary to vitamin D-induced hypercalcemia remain scarce in the literature [12–14]. Here, we describe a case of acute kidney injury caused by iatrogenic vitamin D toxicity and provide a brief review of the topic.
Case Presentation
In December 2024, a 35-year-old male presented for a routine clinical evaluation. Laboratory findings revealed significant renal impairment and electrolyte imbalances, including a serum creatinine of 8.2 mg/dL, urea of 141 mg/dL, calcium levels of 12.6 mg/dL, phosphorus of 5.3 mg/dL, hematocrit 39%, sodium 136 mEq/L, and potassium 5.7 mEq/L. Urinalysis showed a normal sediment and absence of proteinuria. A subsequently obtained Parathyroid Hormone (PTH) level was at 19 pg/mL.
Two weeks prior to presentation, the patient reported a mild, self-limited episode of vomiting and diarrhea. Upon admission, he was clinically euvolemic, with normal blood pressure and preserved urine output. The patient was hospitalized with a diagnosis of Acute Kidney Injury (AKI), and management was initiated with intravenous fluid and furosemide. During a five-day hospital stay, renal function partially recovered, with creatinine and urea levels decreasing to 4.87 mg/dL and 97 mg/dL, respectively. The patient remained normotensive and non-oliguric throughout his stay. He was discharged with instructions to continue oral hydration and furosemide 40 mg/day.
Diagnostic imaging performed during hospitalization included a renal ultrasound, which showed kidneys of preserved morphology and cortical thickness. An abdominal CT scan confirmed normal-size, echogenic kidneys without evidence of hydronephrosis or urinary tract dilation; however, microlithiasis was noted in the right kidney (Figure 1).

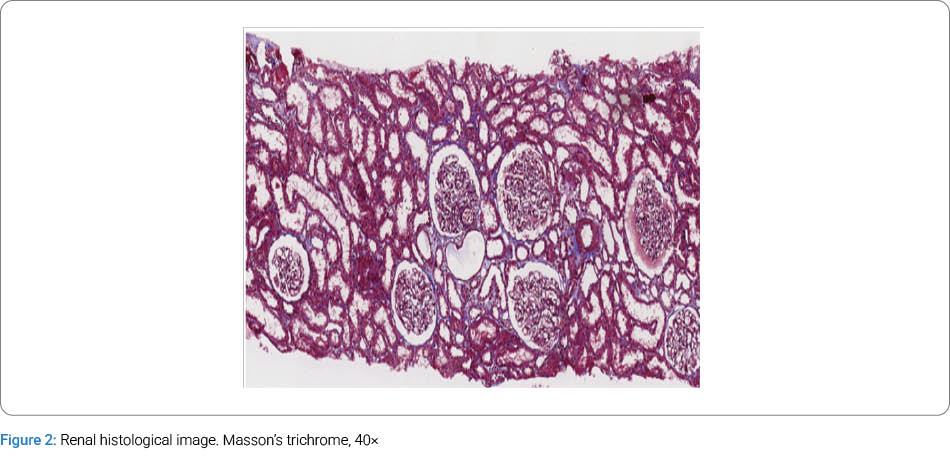
The electrocardiogram was normal with no QT changes. During the clinical course, the 25-hydroxyvitamin D [25(OH)D] level was markedly elevated at 520 ng/mL. Upon further questioning, the patient admitted to self-medicating with an over-the-counter vitamin D3 preparation of uncertain origin, taking 1,000 IU/day for 15 days followed by 5,000 IU/day for an additional 15 days. On January 15, 2025, a renal biopsy was performed. Light microscopy revealed features of Acute Tubular Injury (ATI), characterized by dilated tubular lumina, irregular vacuolization of the tubular cells, and focal detachment or denudation of the lining epithelium. The evaluated glomeruli showed no evidence of global sclerosis or significant architectural alterations. Furthermore, there were no signs of interstitial fibrosis or tubular atrophy. No deposits of calcium crystals or other exogenous substances were identified. Immunofluorescence was negative for all routine markers (IgG, IgA, IgM, C3, C1q, kappa, and lambda) (Figure 2).
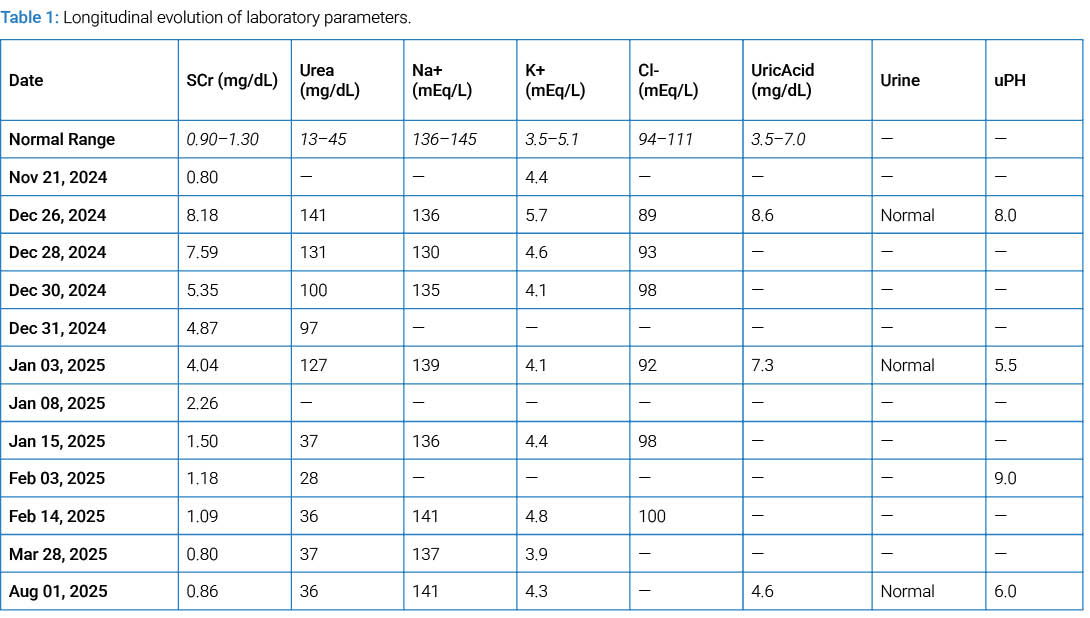
One month post-hospitalization, the 1,25-dihydroxyvitamin D [1,25(OH)2D] level was elevated at 62 pg/mL (normal range: < 52 pg/mL). Following three months of vitamin D supplementation withdrawal, the patient achieved full recovery of renal function. At the eight-month follow-up, the 25(OH)D level had decreased to 90 ng/mL. The longitudinal evolution of renal function parameters and electrolyte levels is summarized in (Table 1).
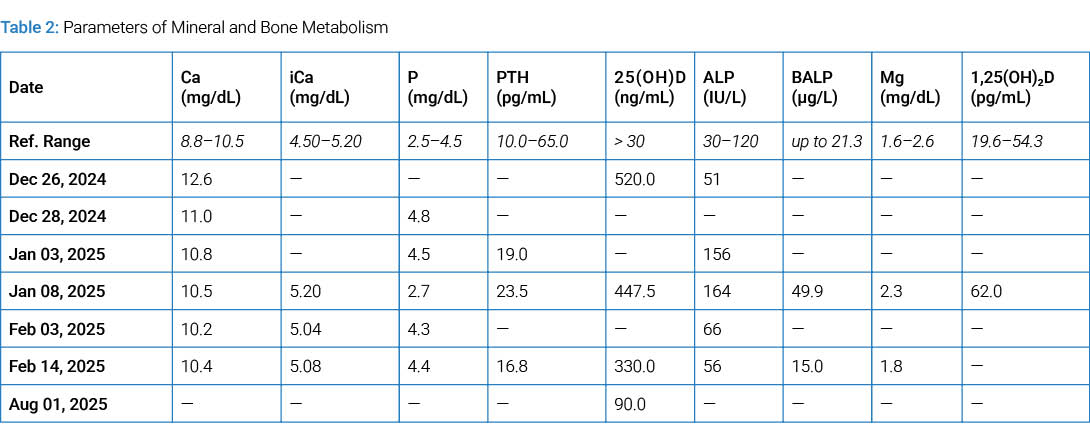
It is noteworthy that the Urinary Albumin-to-Creatinine Ratio (UACR) was within normal limits at 14 mg/g, and the serum albumin level was 4.5 g/dL. The longitudinal evolution of bone and mineral metabolism parameters, including vitamin D metabolites and calcium levels, is summarized in (Table 2).
Discussion
We present a case of severe AKI secondary to hypercalcemia following self-medication with an over-the-counter vitamin D preparation of uncertain origin. Upon discontinuation of the supplement and initiation of supportive therapy, the patient achieved full clinical and biochemical recovery, consistent with previous reports [10].
The diagnosis of vitamin D intoxication was confirmed by markedly elevated 25(OH)D levels (reaching 520 ng/mL), hypercalcemia (up to 12.6 mg/dL), and suppressed PTH levels (19 pg/mL). Although the reported dosage (5,000 IU/day) is generally insufficient to induce such profound toxicity, the lack of pharmaceutical control over the product suggests a manufacturing error or a higher-than-labeled concentration, leading to iatrogenic intoxication. Vitamin D toxicity is typically defined by 25(OH)D levels exceeding 150 ng/ mL [15], often resulting from accidental or intentional ingestion of extremely high doses [16–18].
The pathophysiology of hypercalcemia in this context is multifactorial. Excessive 25(OH)D can directly activate the Vitamin D Receptor (VDR) without the need to convert to 1,25(OH)₂D. This induces hypercalcemia through increased intestinal calcium absorption and RANKL-mediated osteoclast activation, which promotes bone resorption. This hypercalcemia with suppressed PTH and hypercalciuria confirms the excessive action of vitamin D [19–21]. The resulting hypercalcemia inhibits renal 1α-hydroxylase activity, thereby decreasing conversion to 1,25(OH)₂D [15]. Interestingly, our patient’s 1,25(OH)₂D level was slightly elevated (62 pg/mL); this does not contradict the diagnosis of exogenous intoxication. In these cases, 1,25(OH)₂D may be normal or slightly elevated due to a decoupling of physiological control: hypercalcemia should inhibit 1α-hydroxylase and reduce 1,25(OH)₂D, but this mechanism may not be immediate or may be ineffective if the substrate level is extremely high [22]. On the other hand, high levels of 25(OH)D can produce analytical interference that slightly overestimates the 1,25(OH)₂D measured by immunoassay [22].
A distinctive feature of this case is the severity of the renal involvement. While hypercalcemia-induced AKI is well-documented, the mechanisms are complex. Hypercalcemia triggers afferent arteriolar vasoconstriction, reducing renal blood flow and the Glomerular Filtration Rate (GFR). This is further exacerbated by the inhibition of nitric oxide-mediated vasodilation [23,24]. Additionally, high calcium levels interfere with vasopressin action in the collecting duct, potentially causing nephrogenic diabetes insipidus. The resulting polyuria and dehydration further compromise the GFR [15,23,24]. For this reason, as in our case, we must take into account that the use of loop diuretics must be carefully monitored to avoid plasma volume depletion and/or hypotension, To which may possibly lead to a worsening of kidney injury.
The literature describes similar clinical cases. Pirotte et al. [25] reported a case of a 20-year-old patient with toxicity with a magistral preparation with soluble vitamins developing hypercalcemia, elevated 25(OH)D, and developed AKI, which later reversed with appropriate treatment. When analyzing the pharmacological preparation, the excess of vitamin D was confirmed. Another report detailed a 70-year-old patient who consumed for 56 days, doses of 2,000 IU of 25(OH)D plus calcitriol 0.25 mcg per day. It is noteworthy that the patient was diabetic and had a previous creatinine of 1.6 mg/dL and required a few hemodialysis sessions after discontinuing the medication [26].
Hypercalcemia can also lead to the presence of renal lithiasis (as we observed in a CT scan in our patient), nephrocalcinosis, and calcium salt precipitation. Our histological findings demonstrated a predominantly tubular injury without significant calcification, highlighting the direct hemodynamic and cytotoxic impact of acute hypercalcemia [23,24].
Recently, in the Balearic Islands in Spain, the Ministry of Health issued an alert due to an outbreak of vitamin D intoxication in at least 16 people, who were hospitalized for acute kidney failure, hypercalcemia and elevated blood levels of vitamin D. This occurred in healthy people after consuming a dietary supplement with an excess of vitamin D linked to a defective batch, purchased online and without pharmaceutical control [27].
Conclusion
We present a case of severe intoxication with 25(OH)D by apocryphal medication with critical hypercalcemia that led to renal failure due to acute tubular necrosis, confirmed by renal biopsy. This case underscores the potential dangers of over-the-counter products with inadequate pharmaceutical control. We emphasize that prompt clinical intervention—including immediate discontinuation of vitamin D, intravenous saline hydration, and monitored use of loop diuretics—is essential to rapidly reverse this life-threatening condition and ensure the full recovery of renal function.
Key Clinical Message
A 35-year-old patient with no significant medical history presented with acute kidney injury. A renal biopsy was performed and revealed acute tubular necrosis. The renal impairment was secondary to hypercalcemia induced by iatrogenic vitamin D toxicity. The clinical condition resolved following intravenous fluid, electrolyte management, and loop diuretics (furosemide). We report this case and review the current literature.
Patient consent
We have the patient’s informed consent
Conflict of Interest
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Informed consent was obtained for this publication.
References
- Chapuy MC, Pamphile R, Paris E, Kempf C, Schlichting M, Arnaud S, et al. Combined calcium and vitamin D3 supplementation in elderly women: confirmation of reversal of secondary hyperparathyroidism and hip fracture risk: the Decalyos II study. Osteoporos Int 2002;13(3):257–264.
- Reid IR, Bolland MJ, Grey A. Effects of vitamin D supplements on bone mineral density: a systematic review and meta-analysis. Lancet. 2014;383(9912):146–155.
- Lim S, Shin H, Kim MJ, Ahn HY, Kang SM, Yoon JW, et al. Vitamin D inadequacy is associated with significant coronary artery stenosis in a community-based elderly cohort: The Korean Longitudinal Study on Health and Aging. J Clin Endocrinol Metab. 2012;97(1):169–178.
- Delvin E, Souberbielle JC, Viard JP, Salle B. Role of vitamin D in acquired immune and autoimmune diseases. Crit Rev Clin Lab Sci. 2014;51(4):232–247.
- Brewer LC, Michos ED, Reis JP. Vitamin D in atherosclerosis, vascular disease, and endothelial function. Curr Drug Targets. 2011;12(1):54–60.
- Manson JE, Cook NR, Lee IM, Christen W, Bassuk SS, Mora S, et al. Vitamin D supplements and prevention of cancer and cardiovascular disease. N Engl J Med. 2019;380(1):33–44.
- Moulas AN, Vaiou M. Vitamin D fortification of foods and prospective health outcomes. J Biotechnol. 2018;285:91– 101.
- Gummin DD, Mowry JB, Beuhler MC, Spyker DA, Rivers LJ, Feldman R, et al. 2021 annual report of the National Poison Data System© (NPDS) from America’s Poison Centers: 39th annual report. Clin Toxicol (Phila). 2022;60(12):1381–1643.
- Selby PL, Davies M, Marks JS, Mawer EB. Vitamin D intoxication causes hypercalcaemia by increased bone resorption which responds to pamidronate. Clin Endocrinol (Oxf). 1995;43(5):531–536.
- Marcinowska-Suchowierska E, Kupisz-Urbańska M, Łukaszkiewicz J, Płudowski P, Jones G. Vitamin D toxicity-a clinical perspective. Front Endocrinol (Lausanne). 2018;9:550.
- Deluca HF, Prahl JM, Plum LA. 1,25-Dihydroxyvitamin D is not responsible for toxicity caused by vitamin D or 25-hydroxyvitamin D. Arch Biochem Biophys. 2011;505(2):226–230.
- Barth K, Sedivy M, Lindner G, Schwarz C. Successful treatment with denosumab for two cases with hypercalcemia due to vitamin D intoxication and associated acute kidney injury. CEN Case Reports. 2022;11(1):141–145.
- Khan S, Tariq M, Akhtar M, Sibtain Raza M, Manzoor M. The dark side of the sunshine vitamin: a case of acute renal failure and hypercalcaemia from vitamin d overconsumption. Cureus. 2024;16(9):e70237.
- Moysés-Neto M, Guimarães FM, Ayoub FH, Vieira-Neto OM, Costa JAC, Dantas M. Acute renal failure and hypercalcemia. Ren Fail. 2006;28(2):153–159.
- Tebben PJ, Singh RJ, Kumar R. Vitamin D-mediated hypercalcemia: mechanisms, diagnosis, and treatment. Endocr Rev. 2016;37(5):521–547.
- Taylor PN, Davies JS. A review of the growing risk of vitamin D toxicity from inappropriate practice. Br J Clin Pharmacol. 2018;84(6):1121–1127.
- Lee JP, Tansey M, Jetton JG, Krasowski MD. Vitamin d toxicity: a 16-year retrospective study at an academic medical center. Lab Med. 2018;49(2):123–129.
- Giustina A, Bilezikian JP, Adler RA, Banfi G, Bikle DD, Binkley NC, et al. Consensus statement on vitamin d status assessment and supplementation: whys, whens, and hows. Endocr Rev. 2024;45(5):625–654.
- Levita J, Wilar G, Wahyuni I, Bawono LC, Ramadaini T, Rohani R, et al. Clinical toxicology of vitamin d in pediatrics: a review and case reports. Toxics. 2023;11(7):642.
- Thosani S, Hu MI. Denosumab: a new agent in the management of hypercalcemia of malignancy. Future Oncol. 2015;11(21):2865–2871.
- Sun J, Sun B, Wang W, Han X, Liu H, Du J, et al. Histochemical examination of the effects of high-dose 1,25(oh)2d3 on bone remodeling in young growing rats. J Mol Histol. 2016;47(4):389–399.
- Lim K, Thadhani R. Vitamin D Toxicity. J Bras Nefrol. 2020;42(2):238–244.
- Annamalai C, Viswanathan P. Vitamin d and acute kidney injury: a reciprocal relationship. Biomolecules. 2025;15(4):586.
- Rodrigues Tonon C, Lazzarin Silva TAA, Leal Pereira FW, Rios Queiroz DA, Favero Junior EL, Martins D, et al. A review of current clinical concepts in the pathophysiology, etiology, diagnosis, and management of hypercalcemia. Med Sci Monit. 2022;28:e935821-1–e935821-9.
- Pirotte B, Stifkens F, Kaye O, Radermacher L, Putzeys V, Deflandre J, et al. [Hypercalcemia and acute renal failure: a case report of vitamin D intoxication]. Rev Med Liège. 2015;70(1):12–16.
- Guerra V, Vieira Neto OM, Fernandes Laurindo A, Albuquerque de Paula FJ, Neto MM. Hypercalcemia and renal function impairment associated with vitamin D toxicity: case report. J Bras Nefrol. 2016;38(4):466–469.
- Ministry of Social Rights, Consumption and the 2030 Agenda. Alert for the presence of a high amount of vitamin D in supplement food from Spain (Ref. ES2025/374) [Internet]. Madrid: Government of Spain; 2025.
Cite this article
Javier R, Francisco S, del Valle E, Valeria A. Hypercalcemia due to vitamin D toxicity and acute kidney injury. Clinical case and review. Clin Case Rep J. 2026;7(3):1–5.
Keywords
Vitamin D poisoning; Hypercalcemia; Kidney failure
Copyright
© 2026 Spivacow Francisco. This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY-4.0).
