Incidental Detection of Bilateral Adrenal Masses by Point-of-Care Ultrasound Leading to a Diagnosis of Adrenal Lymphoma
* Muhammad Umer Bin Arshad;
Sama Ghaffar;
-
* Muhammad Umer Bin Arshad: Aga Khan University Hospital, Karachi, Pakistan
-
Sama Ghaffar: Nishtar Hospital, Multan, Pakistan
Abstract
Primary adrenal lymphoma is a very rare cause of adrenal masses. In our case, a 52-year-old male presented with hypotension, fever, weight loss, and abnormal labs. To investigate the cause of hypotension, POCUS was performed, revealing bilateral adrenal masses. Subsequently, a formal scan and CT confirmed the presence of bilateral masses with features of malignancy. CT-guided biopsy then confirmed high-grade B-cell lymphoma. Despite these findings and efforts to stabilize the patient, he developed hospital-acquired pneumonia with type 2 respiratory failure. After a prolonged ICU stay, the patient was terminally weaned off. This case highlights the importance of POCUS in early identification of life-threatening conditions, as well as the need to consider rare differential diagnoses in patients with nonspecific presentations.
Introduction
Adrenal masses are relatively rare, with a study showing a prevalence of only 1.4% [1]. Among the incidentally discovered adrenal tumors, about 10%–20% are bilateral [2]. And among these, only 10% are primary adrenal lymphomas [3]. As the evidence suggests, these tumor types are rare, and therefore, the available literature is mostly case reports.
In a study of 50 cases, the median age of Primary adrenal lymphomas, PAL, was found to be 60.3 years, with the most common type being Diffuse Large B-cell Lymphomas (88%) [4]. The prognosis of the PAL is poor, with a 3-year overall survival rate of 39.4% [5]. Given these statistics, early diagnosis is paramount to enable timely management. One such tool for early diagnosis is POCUS.
POCUS is increasingly being used in the emergency department for a variety of reasons, including evaluation of undifferentiated shocks, initial assessment in trauma, and others. During these scans, many incidental findings are being picked up. An editorial by Sara Obeid shows that, depending on the institution, documentation frequency, and level of experience, the percentages of incidental findings range from 1.6% to 26% [6]. Our study provides one such example: an incidental POCUS finding led to the diagnosis of primary bilateral diffuse large B-cell lymphoma.
Case Presentation
A 52-year-old male with a known case of hypertension and diabetes presented to the emergency department with a fever for 15 days, along with chest congestion and significant weight loss. He was advised oral antibiotics for presumed Pneumonia at a nearby clinic; however, the X-ray was unremarkable (Figure 1).

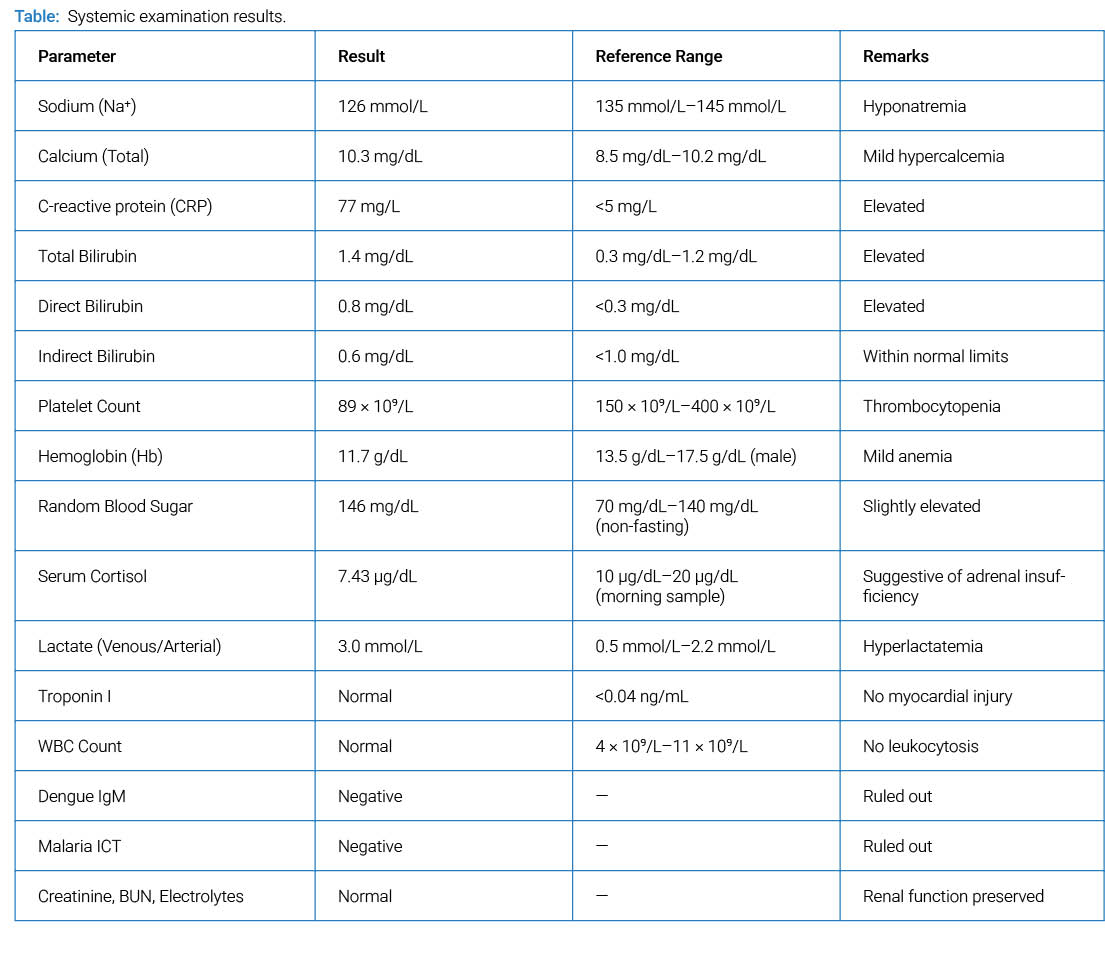
On arrival, he was hypotensive (BP: 83/40 mmHg; MAP: 54 mmHg), tachypneic (RR: 22 breaths/min), but afebrile with a heart rate of 89/min and saturations of 99% on room air. Blood glucose was 146 mg/dL Systemic examination was otherwise unremarkable with no significant findings in cardiovascular, respiratory, gastrointestinal, or neurological examinations (Table).
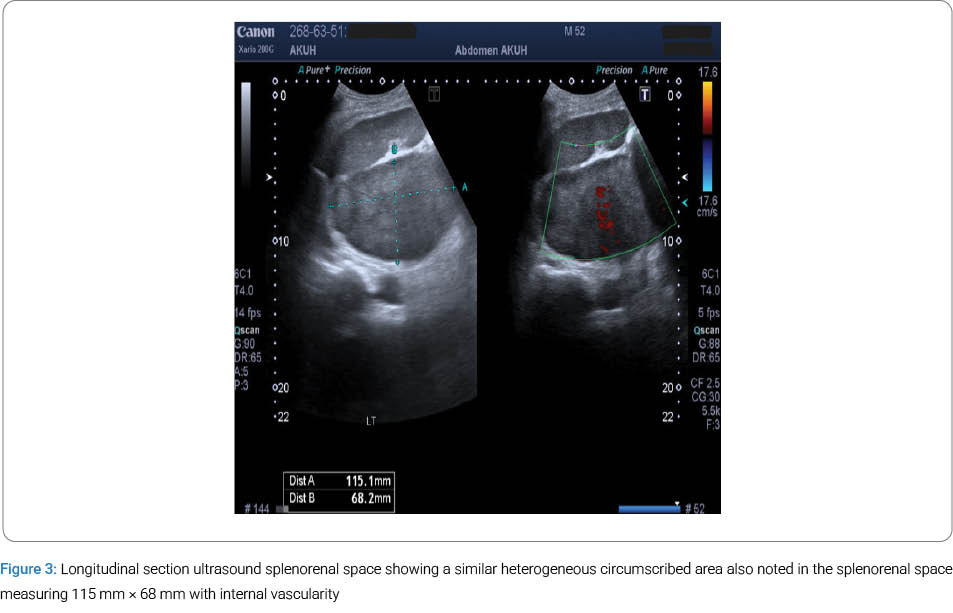
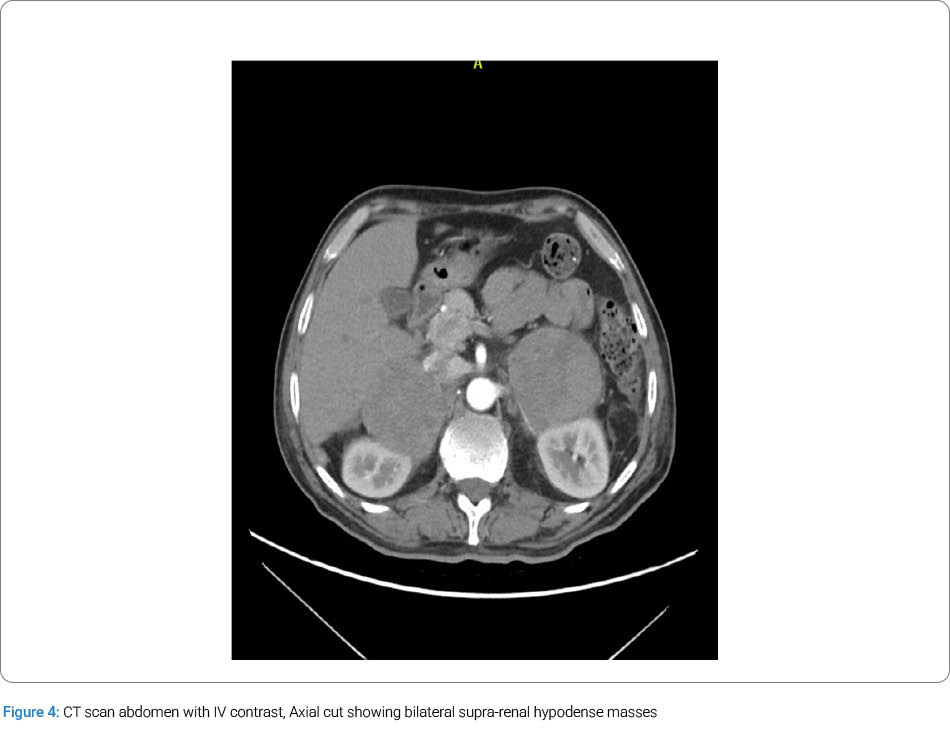
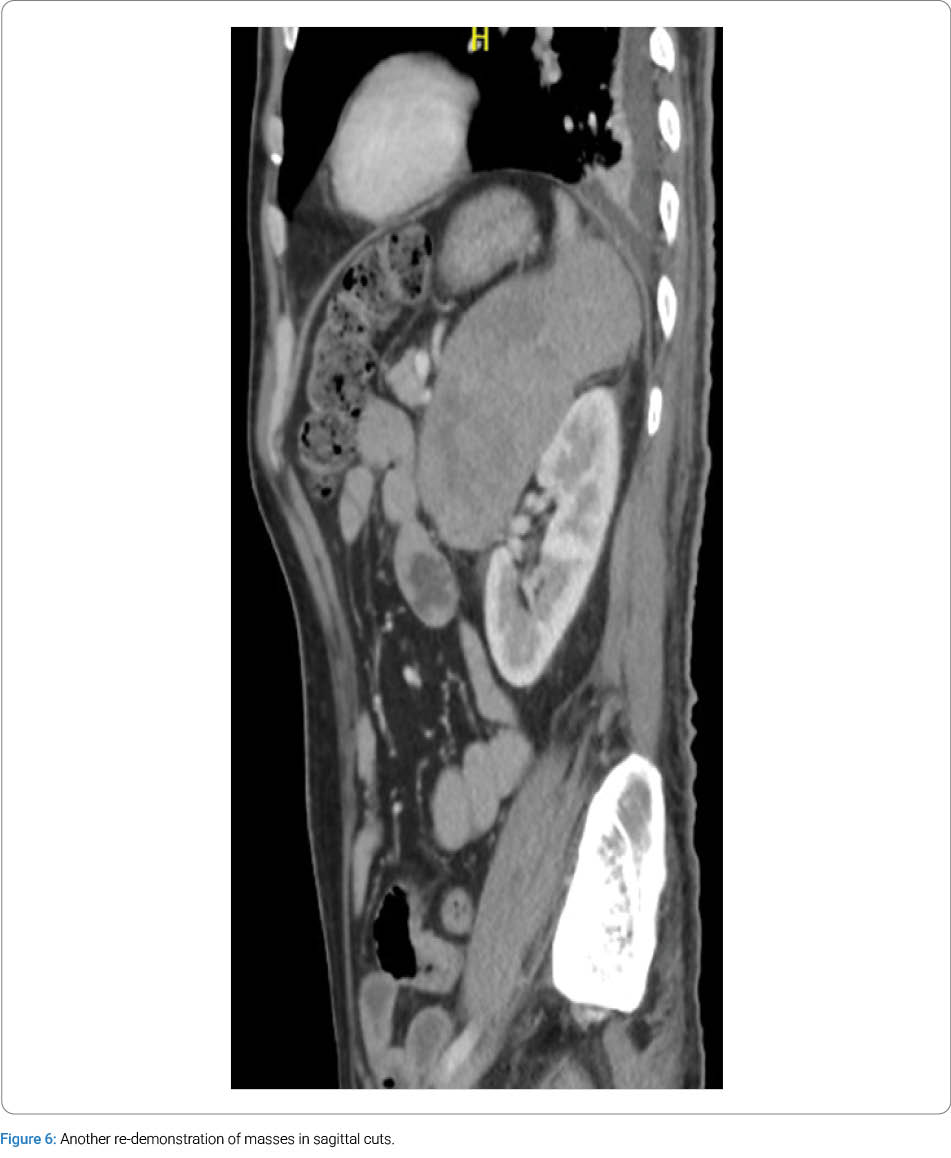
The patient was given IV fluid boluses for hypotension. A point-of-care ultrasound RUSH protocol was performed to evaluate the cause of shock and assess fluid responsiveness, which was estimated as unlikely (Figure 2). In this assessment, bilateral hyperechoic masses were noted in the hypochondrial regions below the liver and spleen, respectively. Follow-up ultrasound of the department confirmed these findings, and subsequent contrast-enhanced CT showed large, bilaterally heterogeneously enhancing adrenal masses with central necrosis, suggesting neoplastic lesions (Figure 3). Early-morning serum cortisol was 7.43 μg/dL, suggestive of adrenal insufficiency. A CT-guided biopsy of the left adrenal mass was done, which showed high-grade B-cell lymphoma (Figure 4).

Unfortunately, during the hospital stay, the patient developed hospital-acquired pneumonia, complicated by type 2 respiratory failure (Figure 5). Resuscitation and management attempts were made, including the use of empirical antibiotics, non-invasive positive pressure ventilation, and finally mechanical ventilation, but the patient showed no improvement, and after discussion with the family, the patient was withdrawn from the ventilator and expired shortly thereafter (Figure 6).

Discussion
In our case, the patient did not undergo a PET scan or a CT chest, so the Diffuse large B-cell lymphoma can be primary or secondary, although history, examination, and investigations make it more likely to be primary than secondary, which is a rarer presentation as compared to the secondary one [7].
Primary DLBCL has a poor prognosis, with a mini review showing that 90% of patients do not live to see another year. This review also talks about indicators of worse prognosis, including high tumor load, advanced age at diagnosis, presence of adrenal insufficiency, and raised LDH [8], and some of these predictors were also present in our case, which explains the outcome of this patient. Another important consideration is that Primary DLBCL often presents in a very non-specific way, as mentioned in the above-mentioned mini review, that the patient can present with just lumbar pain or other vague symptoms such as fever, anemia, hypercalcemia, thrombocytopenia, and weight loss, which is true for this case as well [8]. The combination of rarity and non-specific presentation makes timely diagnosis particularly challenging, which can potentially further worsen the prognosis of a disease that is already associated with poor outcomes.
In cases where rarity and nonspecific presentation coexist, POCUS is very useful for obtaining information at the bedside with almost no side effects. POCUS has well-established clinical utility with protocols such as FAST and RUSH improving patient outcomes. Over the years, it has incidentally picked up findings that have led to rare diagnoses, and our case exemplifies this. There are other similar case reports, such as emphysematous pyelonephritis [9] and gastric volvulus [10], both detected by POCUS. These reports underscore the clinical utility of POCUS. They are evident that POCUS has broader implications than previously recognized. It can even be used as an extension to clinical examination, as suggested by Wong in his case report [11]. The findings from these assessments can then lead to further investigations, such as CT scans, to reach the final diagnosis presented in our case.
POCUS has other benefits as well. Not only does a bedside scan like this not require additional technicians, but it is also less time-consuming, cheaper, and safer as compared to a CT scan, and it is also comparable in terms of diagnostic yield, with multiple studies vouching for its effectiveness and safety [12,13]. Another study has demonstrated that using ultrasound as an initial imaging modality with CT reserved for cases requiring further clarification can lead to lower radiation exposure as compared to using CT as an initial imaging modality in all cases [14]. These studies further support the role of ultrasound as a practical screening tool in situations of diagnostic uncertainty, particularly when the index of suspicion is low or when rare but important conditions need to be ruled out.
This case underscores the importance of considering rare diseases in the differential diagnosis of patients presenting with nonspecific symptoms. Point-of-care ultrasound (POCUS) served as a valuable adjunct in this case, providing rapid bedside information that contributed to early diagnostic suspicion. Clinicians should remain vigilant for rare etiologies and utilize POCUS as a supportive tool in the evaluation of diagnostically challenging presentations.
Acknowledgments
- ChatGPT (OpenAI) was used solely for grammar correction, formatting in accordance with BMJ Case Reports guidelines, and structural refinement of the manuscript. All clinical content, interpretation, and final editing were performed and approved exclusively by the authors.
- We thank the patient and family for their consent to share this case.
- We would also like to appreciate the efforts of the Emergency Department of Aga Khan University Hospital, along with Radiology, Internal Medicine, and ICU departments, in the management of this case.
Funding: This research received no external funding.
Consent: Informed consent was obtained from the patient’s family.
Guarantor: Muhammad Umer Bin Arshad.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Ebbehoj A, Li D, Kaur RJ, Zhang C, Singh S, Li T, et al. Epidemiology of adrenal tumours in Olmsted County, Minnesota, USA: a population-based cohort study. Lancet Diabetes Endocrinol. 2020;8(11):894–902.
- Sweeney AT, Hamidi O, Dogra P, Athimulam S, Correa R, Blake MA, et al. Clinical review: the approach to the evaluation and management of bilateral adrenal masses. Endocr Pract. 2024;30(10):987–1002.
- Lomte N, Bandgar T, Khare S, Jadhav S, Lila A, Goroshi M, et al. Bilateral adrenal masses: a single-centre experience. Endocr Connect. 2016;5(2):92–100.
- Wang Y, Ren Y, Ma L, Li J, Zhu Y, Zhao L, et al. Clinical features of 50 patients with primary adrenal lymphoma. Front Endocrinol (Lausanne). 2020;11:595.
- Majidi F, Martino S, Kondakci M, Antke C, Haase M, Chortis V, et al. Clinical spectrum of primary adrenal lymphoma: results of a multicenter cohort study. Eur J Endocrinol. 2020;183(4):453–462.
- Obeid S, Galen B, Jensen T. Incidental findings in POCUS: “Chance favors the prepared mind”. Pocus J. 2022;7(1):113–114.
- Torres F, Suárez U, Pizano P. Diffuse large B-cell lymphoma presenting as acute adrenal hemorrhage. Blood Res. 2025;60(1):18.
- Rezkallah EMN, Hanna RS, Elsaify WM. Adrenal lymphoma: case reports and mini-review. Int J Endocrinol Metab. 2022;20(4):e128386.
- Irish endocrine society 44th annual meeting. Ir J Med Sci. 2021;190(Suppl 3):77–115.
- Xing ZX, Yang H, Zhang W, Wang Y, Wang CS, Chen T, et al. Point-of-care ultrasound for the early diagnosis of emphysematous pyelonephritis: a case report and literature review. World J Clin Cases. 2021;9(11):2584–2594.
- Kitai Y, Sato R, Inoue T. Gastric volvulus suspected by POCUS finding in the emergency department. BMJ Case Rep. 2022;15(8):e250659.
- Wong TC, Tan RC, Lu JX, Cheng TH, Lin WJ, Chiu TF, et al. Point-of-care ultrasonography as an extension of the physical examination for abdominal pain in the emergency department: the diagnosis of small-bowel volvulus as a rare complication after changing the feeding jejunostomy tube. Diagnostics (Basel). 2022;12(5):1153.
- Obernauer J, Galiano K, Gruber H, Bale RJ, Obwegeser AA, Schatzer R, et al. Ultrasound-guided versus computed tomography-controlled facet joint injections in the middle and lower cervical spine: a prospective randomized clinical trial. Med Ultrason. 2013;15(1):10–15.
- Smith-Bindman R, Aubin C, Bailitz J, Bengiamin RN, Camargo CA, Corbo J, et al. Ultrasonography versus computed tomography for suspected nephrolithiasis. N Engl J Med. 2014;371(12):1100–1110.
Cite this article
Bin Arshad MU, Ghaffar S. Incidental Detection of Bilateral Adrenal Masses by Point-of-Care Ultrasound Leading to a Diagnosis of Adrenal Lymphoma. Clin Case Rep J. 2026;7(3):1–5.
Keywords
POCUS; Adrenal lymphoma; High-Grade B-Cell Lymphoma; Adrenal insufficiency; Hypotension
Copyright:
© 2026 Muhammad Umer Bin Arshad. This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY-4.0).
