Post-diphtheritic Bilateral Vocal Fold Palsy: A Case Report
* Walczuk N;
El Ayoubi M;
Verhasselt M;
Rodriguez A;
Dequanter D;
Cavelier G;
-
* Walczuk N: Department of Otorhinolaryngology and Head and Neck Surgery, CHU Saint-Pierre, Belgium
-
El Ayoubi M: Department of Otorhinolaryngology and Head and Neck Surgery, CHU Saint-Pierre, Belgium
-
Verhasselt M: Department of Otorhinolaryngology and Head and Neck Surgery, CHU Saint-Pierre, Belgium
-
Rodriguez A: Department of Otorhinolaryngology and Head and Neck Surgery, CHU Saint-Pierre, Belgium
-
Dequanter D: Department of Otorhinolaryngology and Head and Neck Surgery, CHU Saint-Pierre, Belgium,Department of Stomatology and Maxillofacial Surgery, CHU Saint-Pierre, Belgium
-
Cavelier G: Department of Otorhinolaryngology and Head and Neck Surgery, CHU Saint-Pierre, Belgium,Department of Otorhinolaryngology and Head and Neck Surgery, Hôpital Universitaire des Enfants Reine Fabiola, Belgium
-
Jul 13, 2026 |
-
Volume: 7 |
-
Issue: 3 |
-
Views: 273 |
-
Downloads: 427 |
Abstract
Introduction: Diphtheria is a rare infectious disease caused by toxin-producing Corynebacterium diphtheriae. While vaccination has led to a global decline, it remains endemic in areas with inadequate immunization and is predominantly identified among travelers and migrants within the European Union (EU). Systemic complications, such as myocarditis and demyelinating polyneuropathy, are caused by the Diphtheria toxin (DT), which inhibits protein synthesis. While cranial nerve involvement is a recognized feature, bilateral vocal fold palsy in abduction represents an exceptionally rare and highly disabling neurological manifestation.
Clinical Case: A 59-year-old partially vaccinated woman developed severe respiratory diphtheria complicated by myocarditis and a delayed sensorimotor polyneuropathy. Clinical evaluation and Fiberoptic Endoscopic Evaluation of Swallowing revealed palatal palsy and bilateral vocal fold palsy in abduction, resulting in aphonia and profound dysphagia. Due to persistent vocal fold atrophy and glottic insufficiency, an autologous fat injection was performed. However, at the two-month follow-up, the patient demonstrated a significant recovery of the initial palsy, leaving only mild residual atrophy.
Conclusion: This case expands the spectrum of diphtheritic neuropathy by documenting the rare complication of bilateral vocal fold palsy in abduction associated with myocarditis and polyneuropathy. The observation of late palsy recovery highlights the importance of waiting at least 9 months from disease onset before considering corrective surgery, as neurological improvement may occur as late as 8 months. This report emphasizes the potential for persistent structural sequelae requiring surgical intervention and underscores the need for vigilant long-term multidisciplinary management of patients with toxin-producing diphtheria. It also underscores the need for widespread vaccination coverage.
Abbreviations
EEA: European Economic Area; ER: Emergency Room EU: European Union; CT: Computed Tomography; DT: Diphteria Toxin; DPT: Diphteria-Pertussis-Tetanus
Introduction
Diphtheria is a rare infectious disease caused by Corynebacterium diphtheriae and exists primarily in respiratory and cutaneous forms [1]. This potentially deadly disease is highly transmissible via respiratory droplets or direct contact with cutaneous lesions [1–4]. The introduction of the trivalent Diphtheria-Pertussis-Tetanus (DPT) vaccine has led to a substantial global decline in the disease. Complemented by adult boosters, it remains the most effective preventive strategy [2]. Since vaccinated people may still be colonized and capable of transmission, vaccination alone is effective in interrupting spread in only 28% of outbreaks, rendering isolation and antibiotic administration critical [5]. Respiratory cases with pseudomembrane carry the greatest mortality [4,6]. Untreated respiratory diphtheria has an estimated 29% case-fatality rate among untreated unvaccinated people [5]. Diphtheria remains endemic and may reach epidemic levels in parts of the world where immunization rates are inadequate. Within the European Union (EU) and European Economic Area (EEA), confirmed cases are predominantly identified in travelers and migrants from these endemic areas [7].
The respiratory form often affects the nasal cavity, pharynx, larynx, and tonsils, producing a pseudomembrane and cervical lymph nodes. It may lead to systemic complications such as myocarditis and neuropathy caused by the Diphtheria toxin (DT). DT is an exotoxin encoded by the tox gene of lysogenic corynebacteriophages and exerts cytotoxic effects by binding the HB-EGF receptor on neural and cardiac cells [8–10]. This way, it inhibits protein synthesis and triggers cell death, potentially causing neurological and cardiac complications [1,8,10]. Neurological complications are proportional to respiratory symptom severity. Between 20% and 68% of symptomatic infections progress to polyneuropathy [9,11]. This condition has often been described as following a biphasic course with cranial nerve function recovering as motor deficits in the limbs and trunk progressively deteriorate [1,9,11]. Recovery from diphtheritic polyneuropathy may begin 2 months–4 months following initial disease and can take up to 8 months after symptom onset [9,12,13]. Cardiac complications occur in 10%–25% of cases, potentially causing irreversible myocardial and valvular damage [14]. Patients diagnosed with diphtheria should undergo follow-up for a period of 3 months–6 months to monitor for potential neurological or cardiac complications [15].
We report a clinical case of bilateral vocal cord palsy occurring post diphtheritic infection caused by a toxinogen secreting Corynobacterium diphtheria. This case illustrates a rare neurological complication and highlights the importance of prolonged monitoring of patients who have suffered from a toxinogen-secreting diphtheria.
Case Presentation
A 59-year-old woman presented to the emergency department with a 7-day history of dysphagia, dyspnea, and productive cough. She had initially consulted her general practitioner, who diagnosed bilateral tonsillitis and oropharyngeal candidiasis. She was prescribed 1000 mg amoxicillin three times daily and nystatin four times daily for seven days with no improvement. Upon arrival at the Emergency Room (ER), she exhibited persistent dysphagia, pharyngeal pain, productive cough, fever, dysphonia, and dyspnea. The patient originated from the Balkans, and her DPT vaccination status was not up to date. Her vital signs were notable for oxygen desaturation down to 80%, requiring noninvasive oxygen therapy. Physical examination revealed cervical lymph nodes and bilateral tonsillitis with white pseudomembranes covering the tonsils and the dorsal tongue. Flexible laryngoscopy showed extension of the pseudomembranes into the nasopharynx and larynx with preserved vocal fold mobility. A cervico-facial Computed Tomography (CT) demonstrated a hypertrophy of the palatine and lingual tonsils, inflammatory thickening of the pre-epiglottic fat, aryepiglottic folds, and epiglottis, along with reactive cervical lymphadenopathies. The patient was transferred to the Intensive Care Unit due to worsening of epiglottitis edema and dyspnea. An oropharyngeal swab taken upon arrival returned positive on day 11 of symptoms for a toxin-producing Corynebacterium diphtheriae and Candida tropicalis. Treatment was initiated with 100,000 IU of diphtheria antitoxin along with intravenous clarithromycin and amoxicillin-clavulanate for 14 days. Between 12 days–21 days of symptoms, serum troponin T levels rose up to 2525.0 ng/dL. Transthoracic echocardiography revealed hypokinesia of the left ventricle, supporting a diagnosis of diphtheritic myocarditis with a decrease in cardiac output. The patient was later discharged after two negative oropharyngeal swabs during the fourth week of the disease. Eight weeks after the onset of symptoms, the patient returned to the ER for recurrent dyspnea and cough. The nasopharyngeal swab tested positive for a SARS-CoV-2 infection. During her hospitalization, a detailed clinical and anamnestic reassessment revealed objective signs consistent with peripheral polyneuropathy, in addition to the symptoms reported by the patient. She presented persistent dysphonia, distal sensory deficits, gait disturbances, and paresthesia of the hands and feet since her previous admission. Tendon reflexes and plantar responses were absent. On day 75 of the disease, a Fiberoptic Endoscopic Evaluation of Swallowing (F.E.E.S.) revealed palatal palsy, bilateral vocal cord palsy in abduction, along with an absence of the pharyngeal phase of swallowing and no cough reflex. Speech-language pathology assessment revealed oral hypoesthesia and ageusia, absence of gag reflex with palatal palsy, and aphonia without compensatory or ventricular phonation. Feeding with a nasogastric tube was then preconized. A cervico-facial CT scan could reasonably exclude an organic cause for the paralysis, and there was no history of endotracheal intubation.
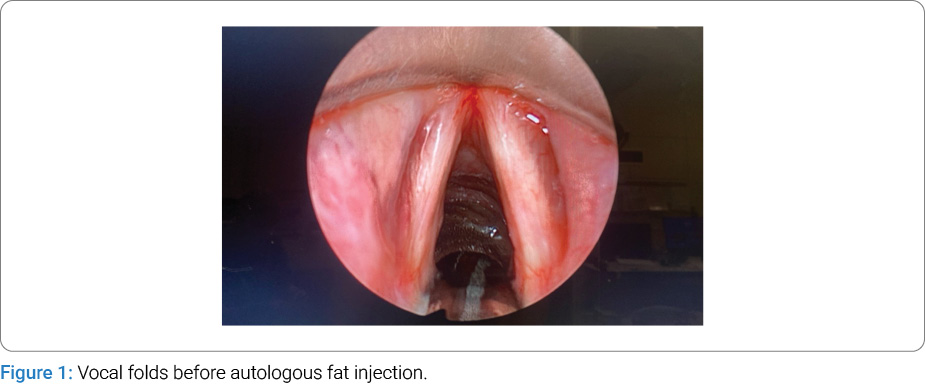
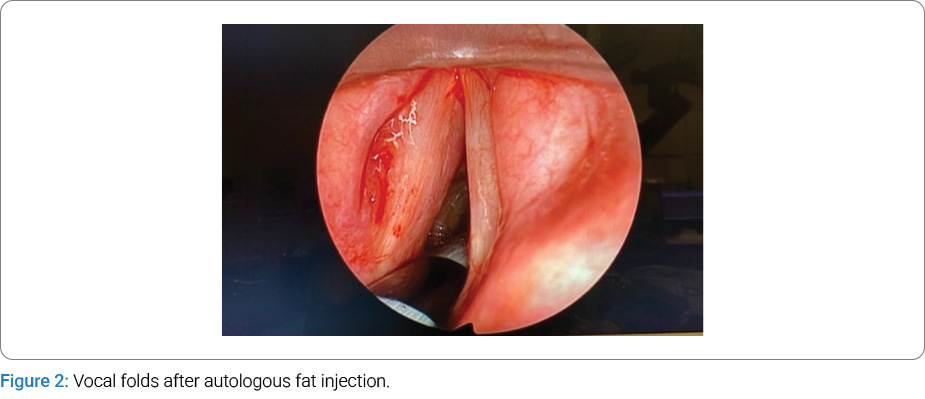
A rehabilitation program was initiated, focusing on swallowing and intraoral sensory stimulation along with physiotherapy. On day 82, electromyography revealed prolonged distal motor latencies, reduced amplitudes, and dispersed responses with preserved motor conduction velocity in both peroneal nerves. Additionally, sensory conduction velocity was slowed, and responses were dispersed in both sural nerves. Chronic neurogenic changes were also observed in the anterior tibialis muscle. These findings supported the diagnosis of a diphtheritic demyelinating sensorimotor polyneuropathy. The patient began a gradual recovery, with a return of swallowing and gag reflexes by day 103. By day 110, the F.E.E.S. demonstrated improved vocal cord mobility, although left vocal cord atrophy persisted, resulting in a glottic gap. Rigid laryngoscopy with lipofilling of the left vocal cord for its medialization was performed on day 163 to improve voice quality and swallowing (Figure 1, Figure 2). Regarding the other complications, transthoracic echocardiography showed complete recovery. However, paresis of the upper and lower limbs remained only partially resolved at last follow-up.
Discussion
Diphtheria is a multisystemic disease in which both acute airway obstruction and delayed neurological and cardiac complications can be life-threatening. Our patient’s clinical presentation suggests involvement of the glossopharyngeal (IX) and vagus (X) nerves, with possible extension to the cranial portion of the accessory nerve (XI). It is remarkable for the development of bilateral vocal fold palsy in abduction, a rare but highly disabling manifestation of diphtheritic neuropathy. While cranial nerve involvement is well recognized, bilateral impairment of recurrent laryngeal nerves with complete vocal fold immobility has rarely been reported [9]. Several studies have reported that the earliest manifestations of DP typically consist of soft palate paresis and distal extremity paresthesia [9,12]. Other complications, such as 3rd to 7th cranial nerve involvement, diaphragmatic palsy, and loss of vasomotor tone, had also been described [13]. The onset of neurological complications in our case report can be estimated between week 2 and week 8 since the beginning of the disease. It has been similarly described to appear between 2 and 50 days by other authors [9,11,12]. The progressive and delayed recovery observed in our patient echoes that reported in previous studies and is likely attributable to the late administration of diphtheria antitoxin, which was initiated only on day 11 of symptoms. The selective and bilateral involvement of the recurrent laryngeal nerves represents a severe form of bulbar neuropathy with immediate consequences for airway safety and vocal function. To our knowledge, only Piradov et al. have reported a similar Xth cranial nerve complication [9]. Unlike the more common palatal and pharyngeal palsies, bilateral vocal fold immobility often requires targeted interventions to maintain adequate breathing and phonation. The persistence of vocal fold atrophy and glottic insufficiency highlights the possibility of permanent sequelae. Autologous fat injection was performed to correct the glottic insufficiency. At the 2-month follow-up, the patient demonstrated recovery from palsy, with only mild residual atrophy of the left vocal fold. This case underscores the importance of waiting at least 9 months from disease onset before considering corrective surgery, given that recovery may occur as late as 8 months. Furthermore, the coexistence of diphtheritic myocarditis in our patient illustrates the systemic nature of the toxin-mediated damage. The combination of cardiac and neurological complications within a short timeframe reflects the severe burden of untreated or late-treated diphtheria, as in our case. This emphasizes the critical importance of early recognition, timely administration of antitoxin, and multidisciplinary management involving infectious disease specialists, neurologists, cardiologists, and otolaryngologists. From 2016 to 2021, the European Center for Disease Prevention and Control (ECDC) recorded an annual mean of 27 reported cases of Corynebacterium diphtheriae infection within the EU and the EEA [7]. While diphtheria is rare in Europe, it can re-emerge in regions with insufficient vaccination coverage. Epidemiological data suggest that many cases involve individuals who migrated through the Western Balkans, the region from which our patient originates. Although childhood vaccination rates remain high in Europe, waning immunity and lower protection in adults may create additional susceptibility, highlighting the relevance of vaccination boosters [7].
Conclusion
This case expands the spectrum of diphtheritic neuropathy by documenting the rare complication of bilateral vocal fold palsy in abduction associated with myocarditis and polyneuropathy. It emphasizes the potential for persistent structural sequelae requiring surgical intervention and underscores the need for vigilant long-term multidisciplinary management of patients with toxin-producing diphtheria. It also underlines the necessity of widespread vaccination.
Conflict of Interest
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Informed consent was obtained for this publication.
References
- Hadfield TL, McEvoy P, Polotsky Y, Tzinserling VA, Yakovlev AA. The pathology of diphtheria. J Infect Dis. 2000;181(Suppl 1): S116–S120.
- World Health Organization. Diphtheria vaccine: WHO position paper, August 2017 - Recommendations. Vaccine. 2018;36(2):199–201.
- Quick ML, Sutter RW, Kobaidze K, Malakmadze N, Nakashidze R, Murvanidze S, et al. Risk factors for diphtheria: a prospective case-control study in the Republic of Georgia, 1995-1996. J Infect Dis. 2000;181(Suppl 1):S121–S129.
- Wagner KS, White JM, Lucenko I, Mercer D, Crowcroft NS, Neal S, et al. Diphtheria in the postepidemic period, Europe, 2000–2009. Emerg Infect Dis. 2012;18(2):217–225.
- Truelove SA, Keegan LT, Moss WJ, Chaisson LH, Macher E, Azman AS, et al. Clinical and epidemiological aspects of diphtheria: A systematic review and pooled analysis. Clin Infect Dis.2020;71(1):89–97.
- Sharma NC, Banavaliker JN, Ranjan R, Kumar R. Bacteriological & epidemiological characteristics of diphtheria cases in & around Delhi -a retrospective study. Indian J Med Res. 2007;126(6):545–552.
- Hoefer A, Seth-Smith H, Palma F, Schindler S, Freschi L, Dangel A, et al. Corynebacterium diphtheriae outbreak in migrant populations in Europe. N Engl J Med. 2025;392(23):2334–2345.
- Collier RJ. Diphtheria toxin: mode of action and structure. Bacteriol Rev. 1975;39(1):54–85.
- Piradov MA, Pirogov VN, Popova LM, Avdunina IA. Diphtheritic Polyneuropathy: Clinical Analysis of Severe Forms. Arch Neurol. 2001;58(9):1438–1442.
- Alekseev VIu, Kaboev OK, Semenova EV, Shcherbakova OG, Filatov MV. [Immunological similarity of diphtheria toxin and EGF receptor]. Tsitologiia. 2010;52(5):364–370.
- Logina I, Donaghy M. Diphtheritic polyneuropathy: a clinical study and comparison with Guillain-Barré syndrome. J Neurol Neurosurg Psychiatry. 1999;67(4):433–438.
- Jammar SK, Sharma S, Agarwal S, Kataria T, Jat PS, Singh SN, et al. Spectrum of neurological outcomes in diphtheria: A case series. Indian J Otolaryngol Head Neck Surg. 2022; 74(Suppl 3):5454–5459.
- Prasad PL, Rai PL. Prospective study of diphtheria for neurological complications.J Pediatr Neurosci. 2018;13(3): 313–316.
- Ledbetter MK, Cannon AB 2nd, Costa AF. The electrocardiogram in diphtheritic myocarditis. Am Heart J. 1964;68(5):599–611.
- Manikyamba D, Satyavani A, Deepa P. Diphtheritic polyneuropathy in the wake of resurgence of diphtheria. J Pediatr Neurosci. 2015;10(4):331–334.
Cite this article
Walczuk N, El Ayoubi M, Verhasselt M, Rodriguez A, Dequanter D, Cavelier G. Post-diphtheritic bilateral vocal fold palsy: a case report. Clin Case Rep J. 2026;7(3):1–4.
Keywords
Corynebacterium diphtheriae; Diphtheritic toxin; Bilateral vocal fold palsy; Diphtheritic polyneuropathy; Bulbar palsy; Recurrent laryngeal nerve neuropathy
Copyright
© 2026 Walczuk N. This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY-4.0).
